Nawrot Ireneusz, Chudziński Witold, Ciąćka Tomasz, Barczyński Marcin, Szmidt Jacek
Department of General, Vascular, and Transplantation Surgery, Medical University of Warsaw, Warsaw, Poland.
Department of Endocrine Surgery, Third Chair of General Surgery, Jagiellonian University Medical College, Cracow, Poland.
Med Sci Monit. 2014 Sep 9;20:1604-12. doi: 10.12659/MSM.890983.
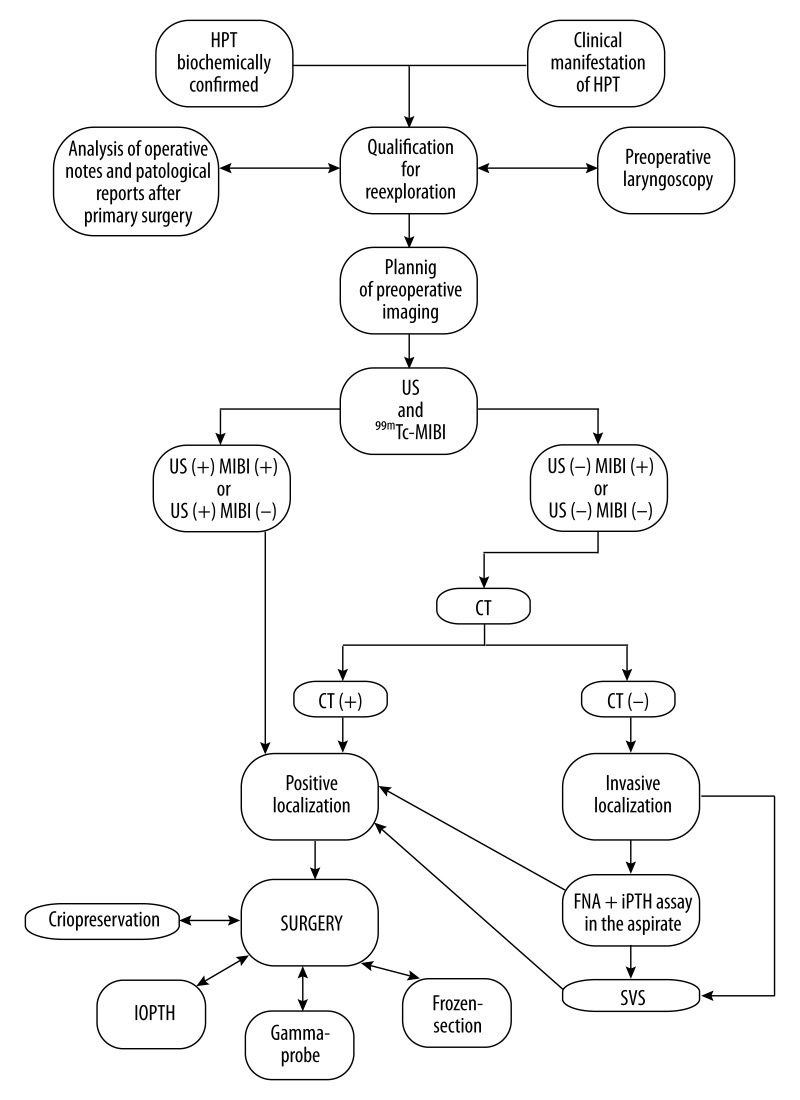
Parathyroid reoperations are challenging and achieving a cure requires multidisciplinary treatment team cooperation. The aims of this study were to summarize our experience in revision surgery for persistent (pHPT) or recurrent primary hyperparathyroidism (rHPT) and to explore factors underlying failure to cure at initial surgery.
This was a retrospective cohort study of patients who underwent reoperations for pHPT or rHPT at a tertiary referral center. The database of parathyroid surgery was searched for eligible patients (treated in the years 2000-2012). The primary outcome was the cure rate. All the patients were followed-up for at least 12 months postoperatively. Factors underlying failure to cure at initial surgery were reviewed based on hospital records.
The study group comprised 88 patients (69 women, 19 men) operated on for persistent (n=57) or recurrent disease (n=31), who underwent 98 reoperations, including 26 (2.4%) patients first operated on at our institution, and 72 (81.8%) patients operated on elsewhere, but referred for revision surgery. A long-term cure was achieved in 83/88 patients (94.3%). The mean post-reoperation follow-up was 91.7 (12-176) months. Missed hyperfunctioning parathyroid gland was found on reoperation in eutopic position in 49 (55.5%) patients, and in ectopic position in 39 (44.3%) patients, including 20 (22.7%) cases of cervical ectopy and 19 (21.6%) cases of mediastinal ectopy.
Multidisciplinary treatment team cooperation at a tertiary referral center, consisting of an accurate preoperative localization, expertise in parathyroid re-explorations, and correct use of intraoperative adjuncts, contribute to the high success rate of parathyroid reoperations.
甲状旁腺再次手术具有挑战性,实现治愈需要多学科治疗团队的合作。本研究的目的是总结我们在持续性(pHPT)或复发性原发性甲状旁腺功能亢进症(rHPT)翻修手术中的经验,并探讨初次手术未能治愈的潜在因素。
这是一项对在三级转诊中心接受pHPT或rHPT再次手术患者的回顾性队列研究。在甲状旁腺手术数据库中搜索符合条件的患者(2000年至2012年接受治疗)。主要结局是治愈率。所有患者术后至少随访12个月。根据医院记录回顾初次手术未能治愈的潜在因素。
研究组包括88例接受持续性(n = 57)或复发性疾病(n = 31)手术的患者(69例女性,19例男性),他们接受了98次再次手术,其中26例(2.4%)患者首次在我们机构接受手术,72例(81.8%)患者在其他地方接受手术,但转诊进行翻修手术。83/88例患者(94.3%)实现了长期治愈。再次手术后的平均随访时间为91.7(12 - 176)个月。再次手术时,49例(55.5%)患者在正常位置发现遗漏的功能亢进甲状旁腺,39例(44.3%)患者在异位位置发现,包括20例(22.7%)颈部异位和19例(21.6%)纵隔异位。
三级转诊中心的多学科治疗团队合作,包括准确的术前定位、甲状旁腺再次探查的专业知识以及术中辅助手段的正确使用,有助于提高甲状旁腺再次手术的成功率。