Keutgen Xavier M, Nilubol Naris, Agarwal Sunita, Welch James, Cochran Craig, Marx Steve J, Weinstein Lee S, Simonds William F, Kebebew Electron
Endocrine Oncology Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA.
Metabolic Diseases Branch, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, MD, USA.
Ann Surg Oncol. 2016 Dec;23(Suppl 5):701-707. doi: 10.1245/s10434-016-5467-x. Epub 2016 Jul 27.
Persistent/recurrent primary hyperparathyroidism (pHPT) occurs frequently in multiple endocrine neoplasia type 1 (MEN1). We assessed the usefulness of intraoperative PTH (IOPTH) and preoperative localizing studies based on the outcome of patients with MEN1-associated pHPT undergoing reoperative surgery.
A retrospective analysis identified MEN1 patients with persistent/recurrent pHPT. Patient outcome was defined as postoperative serum calcium and PTH levels (cured, persistent or recurrent) at last follow-up. Positive predictive value (PPV) was calculated for imaging studies and IOPTH.
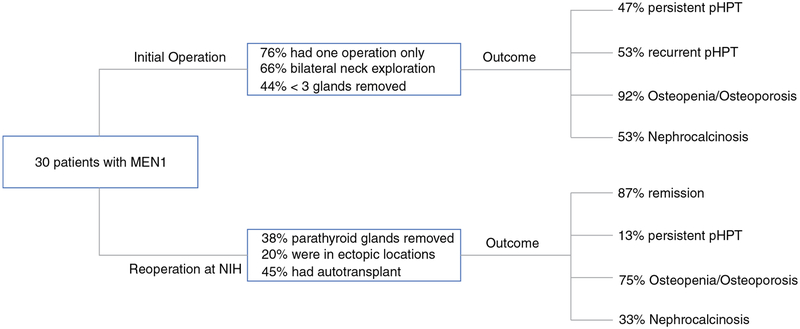
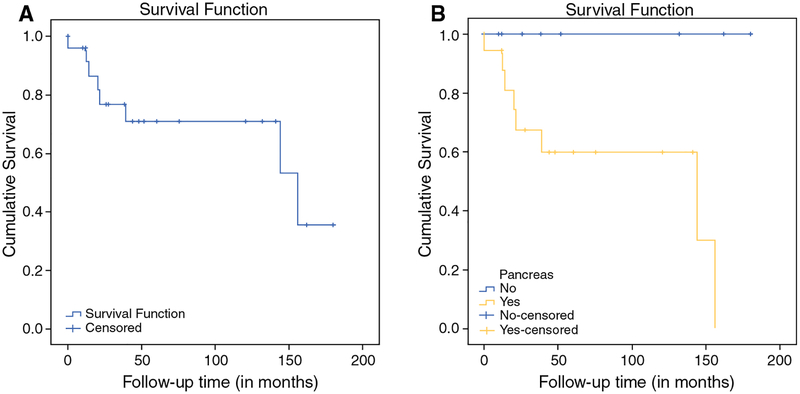
Thirty patients with MEN1-associated recurrent/persistent pHPT underwent 69 reoperative parathyroidectomies. Median follow-up time was 33 months. Persistent pHPT occurred in four (13 %) patients. IOPTH had a 92 % PPV for postoperative eucalcemia. Ultrasound and Tc99m-sestamibi had sensitivities of 100 and 85 % for localizing an enlarged parathyroid gland. However, five (17 %) patients had additional enlarged glands, not visualized preoperatively that were removed after IOPTH did not drop appropriately. Bone mineral density scores did not improve after reoperation (p = 0.60), but the rate of postoperative nephrocalcinosis did (p = 0.046). Patients with pancreatic neuroendocrine tumors had significantly higher rates of persistent/recurrent pHPT compared with those without (40 vs. 0 %, p = 0.021). Intraoperative and delayed parathyroid autotransplantation was performed in nine (30 %) and four (14 %) patients, respectively.
Although preoperative localizing studies are helpful for guiding reoperative strategy in MEN1 with persistent/recurrent pHPT, additional enlarged glands may be missed by conventional imaging. IOPTH should therefore be employed routinely in this setting. Routine cryopreservation should be considered in all patients. Pancreatic manifestation may be associated with earlier recurrence or persistent disease.
持续性/复发性原发性甲状旁腺功能亢进症(pHPT)在1型多发性内分泌腺瘤病(MEN1)中频繁发生。我们基于接受再次手术的MEN1相关pHPT患者的结局,评估了术中甲状旁腺激素(IOPTH)和术前定位研究的效用。
一项回顾性分析确定了患有持续性/复发性pHPT的MEN1患者。患者结局定义为最后一次随访时的术后血清钙和甲状旁腺激素水平(治愈、持续或复发)。计算影像学研究和IOPTH的阳性预测值(PPV)。
30例MEN1相关复发性/持续性pHPT患者接受了69次再次甲状旁腺切除术。中位随访时间为33个月。4例(13%)患者出现持续性pHPT。IOPTH对术后血钙正常的PPV为92%。超声和99m锝-甲氧基异丁基异腈对定位增大的甲状旁腺的敏感性分别为100%和85%。然而,5例(17%)患者有额外增大的腺体,术前未显影,在IOPTH未适当下降后被切除。再次手术后骨密度评分未改善(p = 0.60),但术后肾钙质沉着症的发生率改善了(p = 0.046)。与没有胰腺神经内分泌肿瘤的患者相比,有胰腺神经内分泌肿瘤的患者持续性/复发性pHPT的发生率显著更高(40%对0%,p = 0.021)。分别有9例(30%)和4例(14%)患者进行了术中及延迟甲状旁腺自体移植。
尽管术前定位研究有助于指导MEN1合并持续性/复发性pHPT患者的再次手术策略,但传统影像学检查可能会遗漏额外增大的腺体。因此,在这种情况下应常规使用IOPTH。所有患者均应考虑常规冷冻保存。胰腺表现可能与早期复发或疾病持续存在有关。