Department of Obstetrics and Gynaecology, School of Medicine, University of Nottingham, City Hospital Nottingham, UK.
Front Physiol. 2014 Aug 25;5:310. doi: 10.3389/fphys.2014.00310. eCollection 2014.
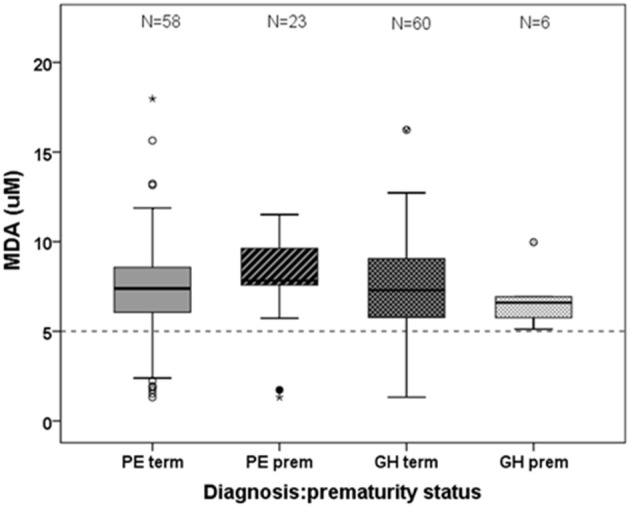
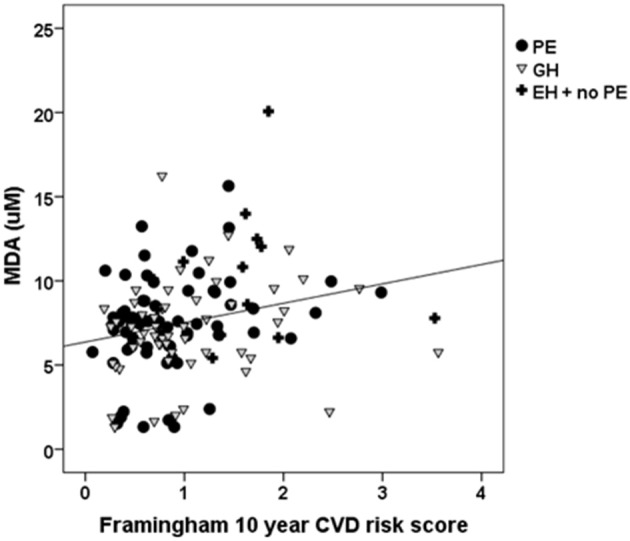
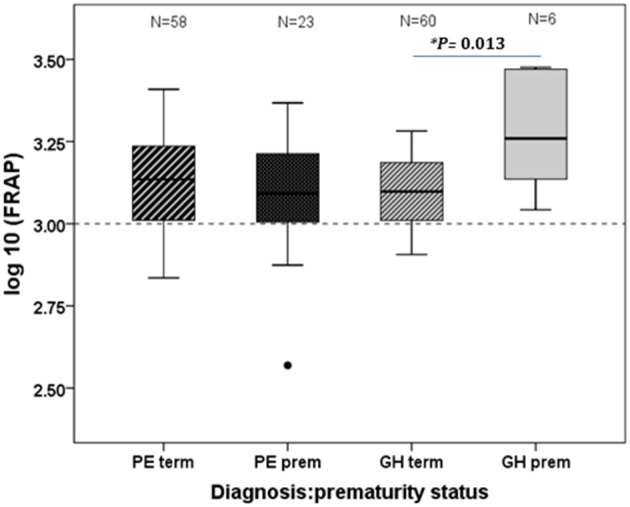
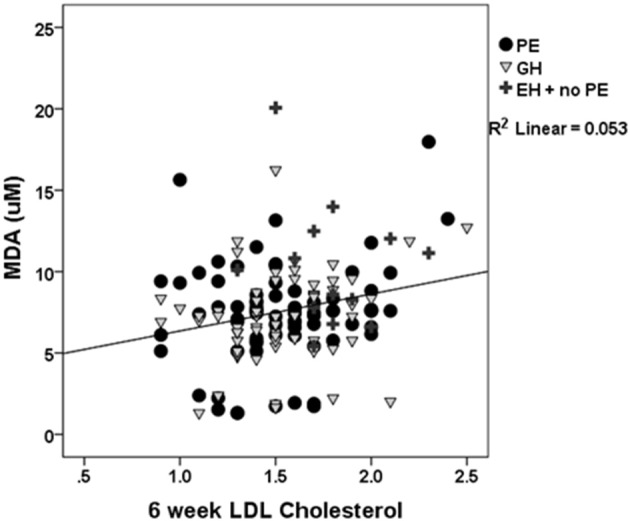
Discussion continues as to whether de novo hypertension in pregnancy with significant proteinuria (pre-eclampsia; PE) and non-proteinuric new hypertension (gestational hypertension; GH) are parts of the same disease spectrum or represent different conditions. Non-pregnant hypertension, pregnancy and PE are all associated with oxidative stress. We have established a 6 weeks postpartum clinic for women who experienced a hypertensive pregnancy. We hypothesized that PE and GH could be distinguished by markers of oxidative stress; thiobarbituric acid reactive substances (TBARS) and antioxidants (ferric ion reducing ability of plasma; FRAP). Since the severity of PE and GH is greater pre-term, we also compared pre-term and term disease. Fifty-eight women had term PE, 23 pre-term PE, 60 had term GH and 6 pre-term GH, 11 pre-existing (essential) hypertension (EH) without PE. Limited data were available from normotensive pregnancies (n = 7) and non-pregnant controls (n = 14). There were no differences in postpartum TBARS or FRAP between hypertensive states; TBARS (P = 0.001) and FRAP (P = 0.009) were lower in plasma of non-pregnant controls compared to recently-pregnant women. Interestingly FRAP was higher in preterm than term GH (P = 0.013). In PE and GH, TBARS correlated with low density lipoprotein (LDL)-cholesterol (P = 0.036); this association strengthened with inclusion of EH (P = 0.011). The 10 year Framingham index for cardiovascular risk was positively associated with TBARS (P = 0.003). Oxidative stress profiles do not differ between hypertensive states but appear to distinguish between recently-pregnant and non-pregnant states. This suggests that pregnancy may alter vascular integrity with changes remaining 6 weeks postpartum. LDL-cholesterol is a known determinant of oxidative stress in cardiovascular disease and we have shown this association to be present in hypertensive pregnancy further emphasizing that such a pregnancy may be revealing a pre-existing cardiovascular risk.
讨论仍在继续,新诊断的妊娠高血压伴有大量蛋白尿(先兆子痫;PE)和非蛋白尿性新高血压(妊娠高血压;GH)是否属于同一疾病谱,或者代表不同的情况。非妊娠高血压、妊娠和 PE 均与氧化应激有关。我们为经历过高血压妊娠的女性设立了一个 6 周产后诊所。我们假设 PE 和 GH 可以通过氧化应激标志物来区分;硫代巴比妥酸反应物质(TBARS)和抗氧化剂(血浆铁离子还原能力;FRAP)。由于 PE 和 GH 的严重程度在早产时更高,我们还比较了早产和足月疾病。58 名女性患有足月 PE、23 名患有早产 PE、60 名患有足月 GH 和 6 名患有早产 GH、11 名患有原发性(特发性)高血压(EH)而无 PE。来自正常血压妊娠(n=7)和非妊娠对照组(n=14)的有限数据。高血压状态之间的产后 TBARS 或 FRAP 无差异;与最近妊娠的女性相比,非妊娠对照组的血浆 TBARS(P=0.001)和 FRAP(P=0.009)更低。有趣的是,与足月 GH 相比,早产 GH 的 FRAP 更高(P=0.013)。在 PE 和 GH 中,TBARS 与低密度脂蛋白(LDL)胆固醇呈正相关(P=0.036);当纳入 EH 时,这种关联增强(P=0.011)。心血管风险的Framingham 指数 10 年预测值与 TBARS 呈正相关(P=0.003)。氧化应激谱在高血压状态之间没有差异,但似乎可以区分最近妊娠和非妊娠状态。这表明妊娠可能改变血管完整性,这种变化在产后 6 周仍然存在。LDL 胆固醇是心血管疾病中氧化应激的已知决定因素,我们已经证明这种关联存在于高血压妊娠中,进一步强调这种妊娠可能揭示了先前存在的心血管风险。