Moja Lorenzo, Lucenteforte Ersilia, Kwag Koren H, Bertele Vittorio, Campomori Annalisa, Chakravarthy Usha, D'Amico Roberto, Dickersin Kay, Kodjikian Laurent, Lindsley Kristina, Loke Yoon, Maguire Maureen, Martin Daniel F, Mugelli Alessandro, Mühlbauer Bernd, Püntmann Isabel, Reeves Barnaby, Rogers Chris, Schmucker Christine, Subramanian Manju L, Virgili Gianni
Department of Biomedical Sciences for Health, University of Milan - IRCCS Galeazzi Orthopaedic Institute, Via Pascal 36, Milan, Italy, 20133.
Cochrane Database Syst Rev. 2014 Sep 15;9(9):CD011230. doi: 10.1002/14651858.CD011230.pub2.
Neovascular age-related macular degeneration (AMD) is the leading cause of legal blindness in elderly populations of industrialised countries. Bevacizumab (Avastin®) and ranibizumab (Lucentis®) are targeted biological drugs (a monoclonal antibody) that inhibit vascular endothelial growth factor, an angiogenic cytokine that promotes vascular leakage and growth, thereby preventing its pathological angiogenesis. Ranibizumab is approved for intravitreal use to treat neovascular AMD, while bevacizumab is approved for intravenous use as a cancer therapy. However, due to the biological similarity of the two drugs, bevacizumab is widely used off-label to treat neovascular AMD.
To assess the systemic safety of intravitreal bevacizumab (brand name Avastin®; Genentech/Roche) compared with intravitreal ranibizumab (brand name Lucentis®; Novartis/Genentech) in people with neovascular AMD. Primary outcomes were death and All serious systemic adverse events (All SSAEs), the latter as a composite outcome in accordance with the International Conference on Harmonisation Good Clinical Practice. Secondary outcomes examined specific SSAEs: fatal and non-fatal myocardial infarctions, strokes, arteriothrombotic events, serious infections, and events grouped in some Medical Dictionary for Regulatory Activities System Organ Classes (MedDRA SOC). We assessed the safety at the longest available follow-up to a maximum of two years.
We searched CENTRAL, MEDLINE, EMBASE and other online databases up to 27 March 2014. We also searched abstracts and clinical study presentations at meetings, trial registries, and contacted authors of included studies when we had questions.
Randomised controlled trials (RCTs) directly comparing intravitreal bevacizumab (1.25 mg) and ranibizumab (0.5 mg) in people with neovascular AMD, regardless of publication status, drug dose, treatment regimen, or follow-up length, and whether the SSAEs of interest were reported in the trial report.
Two authors independently selected studies and assessed the risk of bias for each study. Three authors independently extracted data.We conducted random-effects meta-analyses for the primary and secondary outcomes. We planned a pre-specified analysis to explore deaths and All SSAEs at the one-year follow-up.
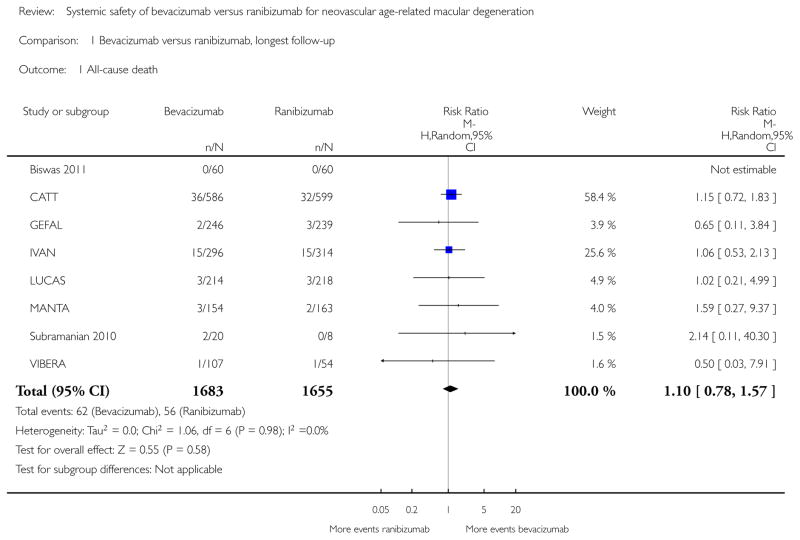
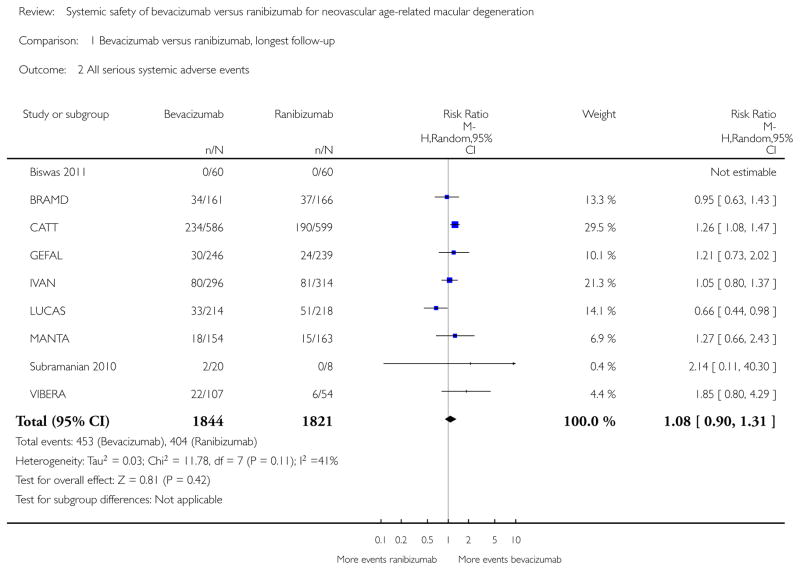
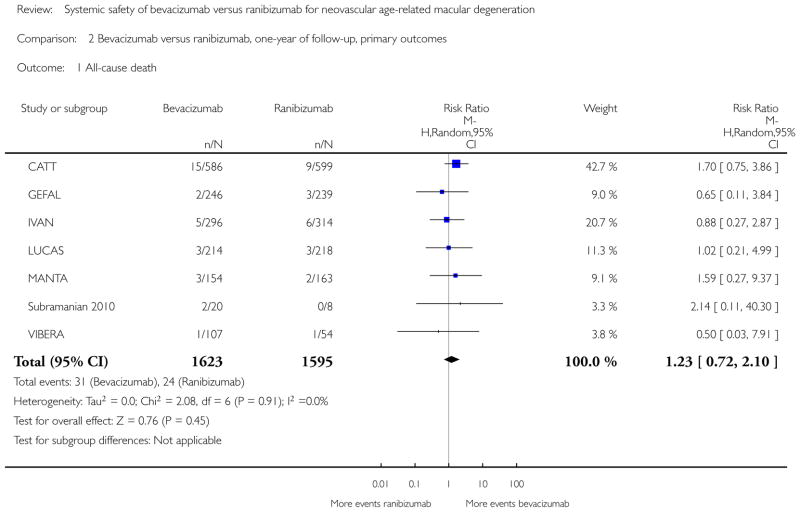
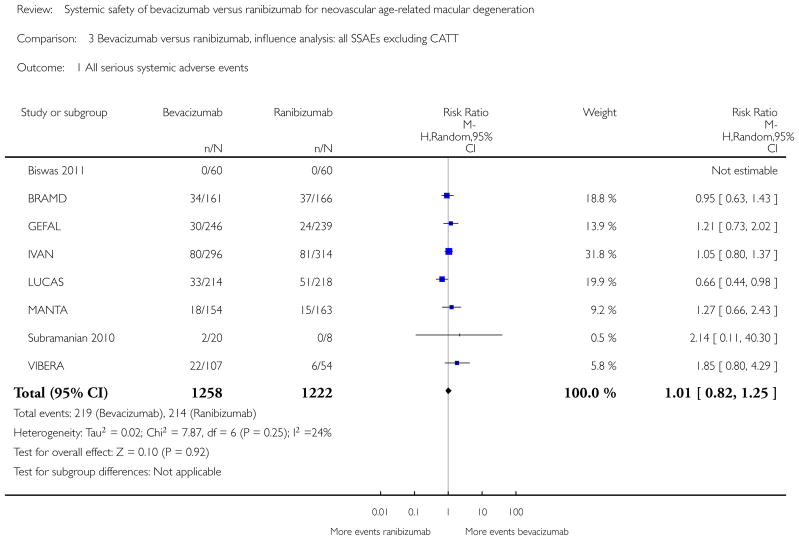
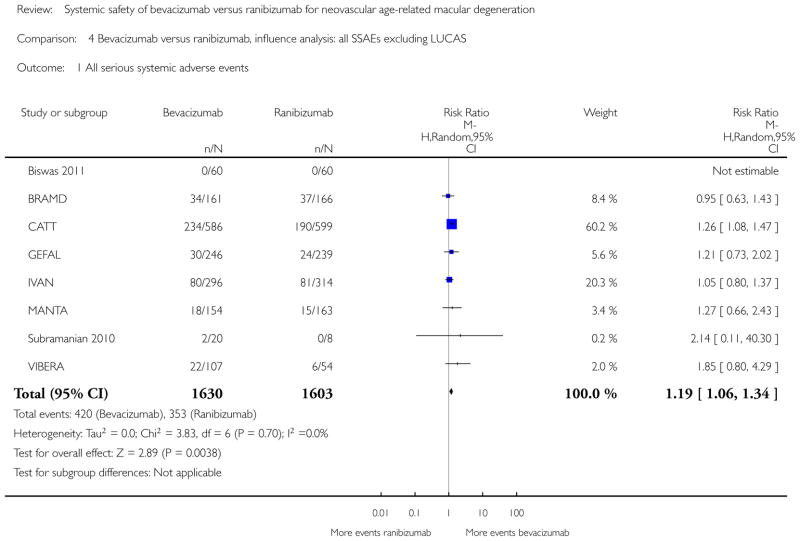
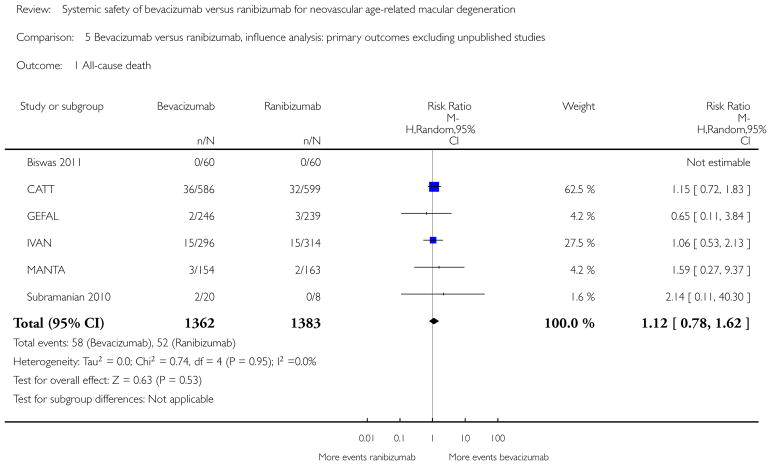
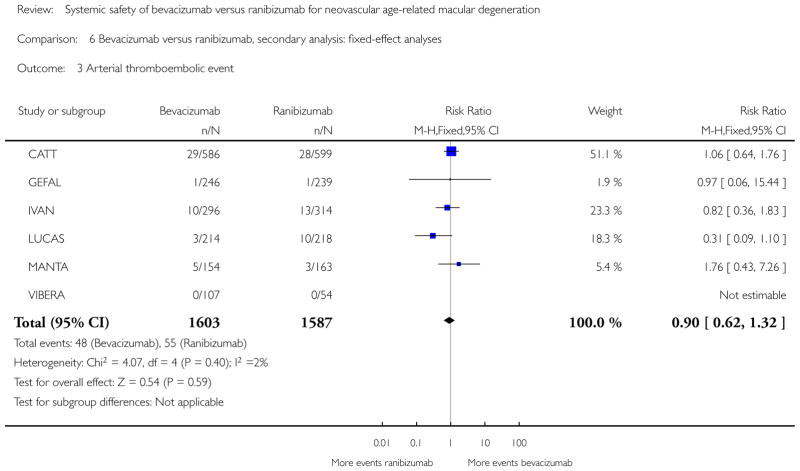
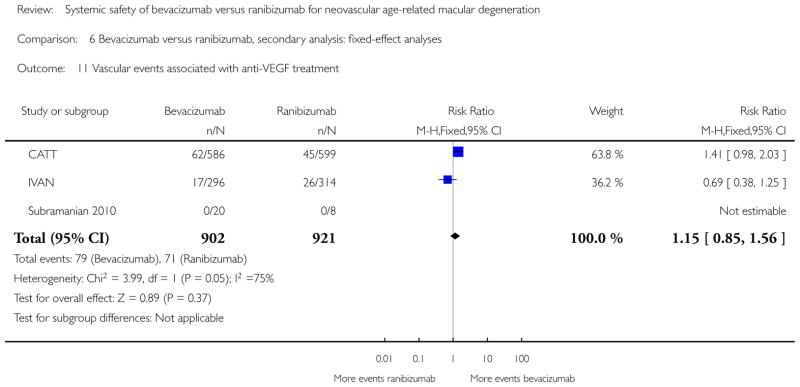
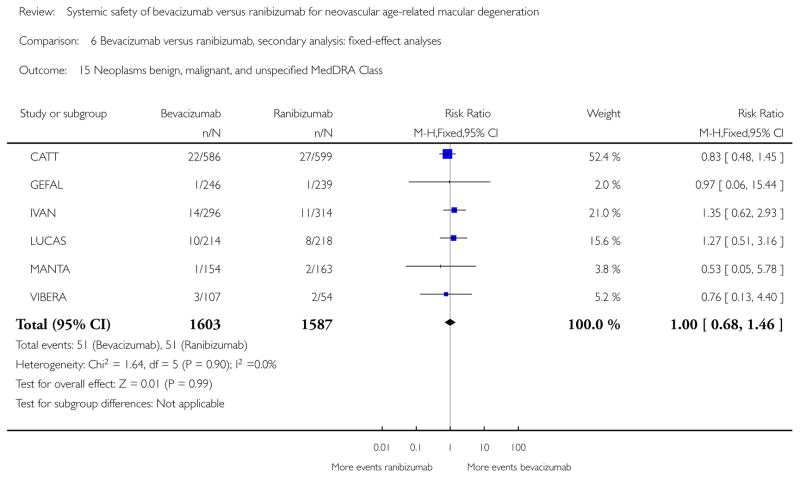
We included data from nine studies (3665 participants), including six published (2745 participants) and three unpublished (920 participants) RCTs, none supported by industry. Three studies excluded participants at high cardiovascular risk, increasing clinical heterogeneity among studies. The studies were well designed, and we did not downgrade the quality of the evidence for any of the outcomes due to risk of bias. Although the estimated effects of bevacizumab and ranibizumab on our outcomes were similar, we downgraded the quality of the evidence due to imprecision.At the maximum follow-up (one or two years), the estimated risk ratio (RR) of death with bevacizumab compared with ranibizumab was 1.10 (95% confidence interval (CI) 0.78 to 1.57, P value = 0.59; eight studies, 3338 participants; moderate quality evidence). Based on the event rates in the studies, this gives a risk of death with ranibizumab of 3.4% and with bevacizumab of 3.7% (95% CI 2.7% to 5.3%).For All SSAEs, the estimated RR was 1.08 (95% CI 0.90 to 1.31, P value = 0.41; nine studies, 3665 participants; low quality evidence). Based on the event rates in the studies, this gives a risk of SSAEs of 22.2% with ranibizumab and with bevacizumab of 24% (95% CI 20% to 29.1%).For the secondary outcomes, we could not detect any difference between bevacizumab and ranibizumab, with the exception of gastrointestinal disorders MedDRA SOC where there was a higher risk with bevacizumab (RR 1.82; 95% CI 1.04 to 3.19, P value = 0.04; six studies, 3190 participants).Pre-specified analyses of deaths and All SSAEs at one-year follow-up did not substantially alter the findings of our review.Fixed-effect analysis for deaths did not substantially alter the findings of our review, but fixed-effect analysis of All SSAEs showed an increased risk for bevacizumab (RR 1.12; 95% CI 1.00 to 1.26, P value = 0.04; nine studies, 3665 participants): the meta-analysis was dominated by a single study (weight = 46.9%).The available evidence was sensitive to the exclusion of CATT or unpublished results. For All SSAEs, the exclusion of CATT moved the overall estimate towards no difference (RR 1.01; 95% CI 0.82 to 1.25, P value = 0.92), while the exclusion of LUCAS yielded a larger RR, with more SSAEs in the bevacizumab group, largely driven by CATT (RR 1.19; 95% CI 1.06 to 1.34, P value = 0.004). The exclusion of all unpublished studies produced a RR of 1.12 for death (95% CI 0.78 to 1.62, P value = 0.53) and a RR of 1.21 for SSAEs (95% CI 1.06 to 1.37, P value = 0.004), indicating a higher risk of SSAEs in those assigned to bevacizumab than ranibizumab.
AUTHORS' CONCLUSIONS: This systematic review of non-industry sponsored RCTs could not determine a difference between intravitreal bevacizumab and ranibizumab for deaths, All SSAEs, or specific subsets of SSAEs in the first two years of treatment, with the exception of gastrointestinal disorders. The current evidence is imprecise and might vary across levels of patient risks, but overall suggests that if a difference exists, it is likely to be small. Health policies for the utilisation of ranibizumab instead of bevacizumab as a routine intervention for neovascular AMD for reasons of systemic safety are not sustained by evidence. The main results and quality of evidence should be verified once all trials are fully published.
新生血管性年龄相关性黄斑变性(AMD)是工业化国家老年人群法定失明的主要原因。贝伐单抗(阿瓦斯汀®)和雷珠单抗(Lucentis®)是靶向生物药物(一种单克隆抗体),可抑制血管内皮生长因子,这是一种促进血管渗漏和生长的血管生成细胞因子,从而防止其病理性血管生成。雷珠单抗被批准用于玻璃体内注射治疗新生血管性AMD,而贝伐单抗被批准用于静脉注射作为癌症治疗药物。然而,由于这两种药物的生物学相似性,贝伐单抗被广泛用于治疗新生血管性AMD的非标签用药。
评估玻璃体内注射贝伐单抗(商品名阿瓦斯汀®;基因泰克/罗氏公司)与玻璃体内注射雷珠单抗(商品名Lucentis®;诺华/基因泰克)在新生血管性AMD患者中的全身安全性。主要结局是死亡和所有严重全身不良事件(All SSAEs),后者是根据国际协调会议的良好临床实践作为综合结局。次要结局检查特定的严重全身不良事件:致命和非致命性心肌梗死、中风、动脉血栓形成事件、严重感染,以及在一些《药物监管活动医学词典》系统器官分类(MedDRA SOC)中分组的事件。我们在最长两年的可用随访期评估安全性。
我们检索了截至2014年3月27日的CENTRAL、MEDLINE、EMBASE和其他在线数据库。我们还检索了会议摘要和临床研究报告、试验注册库,并在有疑问时联系纳入研究的作者。
直接比较玻璃体内注射贝伐单抗(1.25毫克)和雷珠单抗(0.5毫克)治疗新生血管性AMD患者的随机对照试验(RCT),无论其发表状态、药物剂量、治疗方案或随访时间长短,以及试验报告中是否报告了感兴趣的严重全身不良事件。
两位作者独立选择研究并评估每项研究的偏倚风险。三位作者独立提取数据。我们对主要和次要结局进行随机效应荟萃分析。我们计划进行一项预先指定的分析,以探讨一年随访时的死亡和所有严重全身不良事件。
我们纳入了9项研究(3665名参与者)的数据,包括6项已发表研究(2745名参与者)和3项未发表研究(920名参与者)的随机对照试验,均无行业资助。3项研究排除了心血管风险高的参与者,增加了研究间的临床异质性。这些研究设计良好,我们没有因偏倚风险而降低任何结局的证据质量。尽管贝伐单抗和雷珠单抗对我们结局的估计效应相似,但由于不精确性,我们降低了证据质量。在最长随访期(一年或两年),与雷珠单抗相比,贝伐单抗治疗死亡的估计风险比(RR)为1.10(95%置信区间(CI)0.78至1.