Taylor Bradley K, Corder Gregory
Department of Physiology, School of Medicine, University of Kentucky Medical Center, Lexington, KY, 40536-0298, USA,
Curr Top Behav Neurosci. 2014;20:283-325. doi: 10.1007/7854_2014_351.
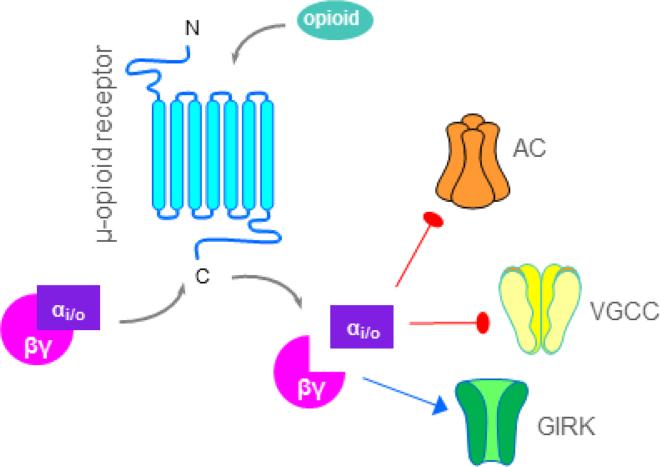
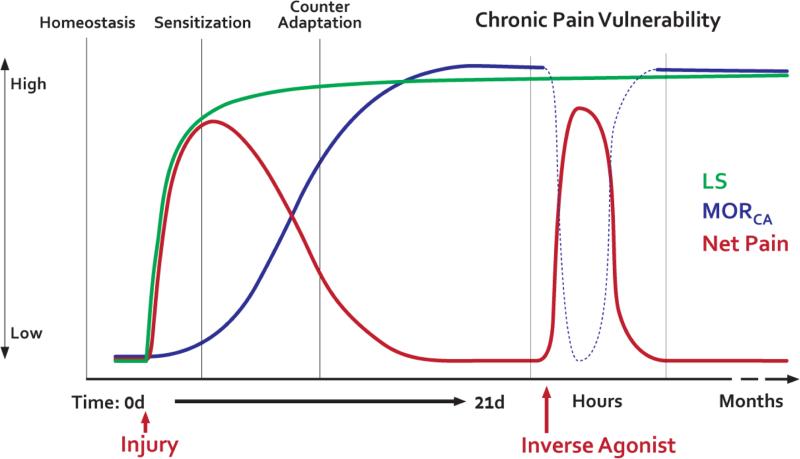
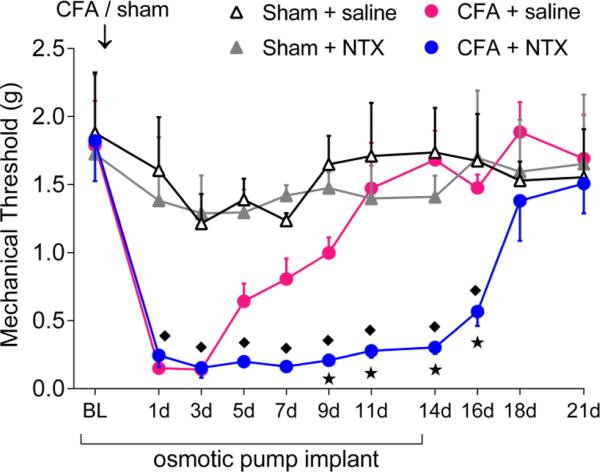
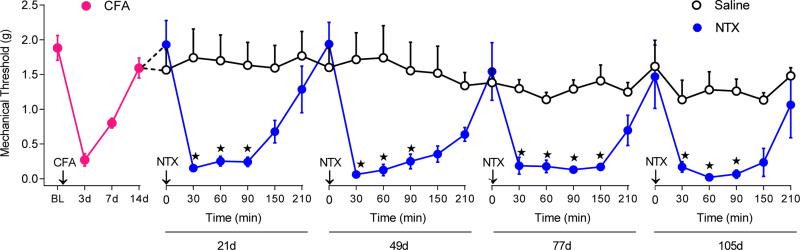
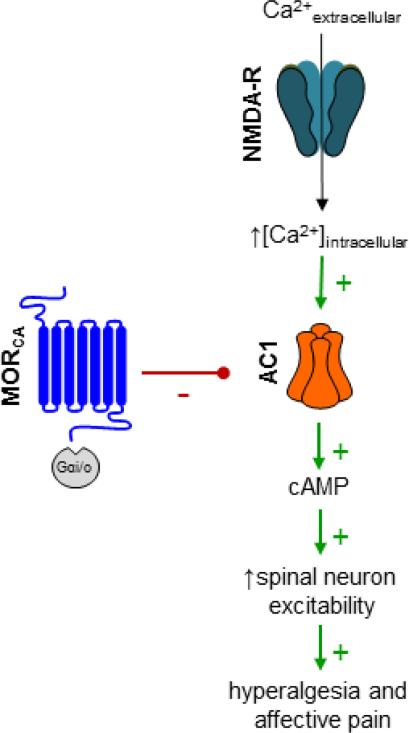
Endogenous activation of µ-opioid receptors (MORs) provides relief from acute pain. Recent studies have established that tissue inflammation produces latent pain sensitization (LS) that is masked by spinal MOR signaling for months, even after complete recovery from injury and re-establishment of normal pain thresholds. Disruption with MOR inverse agonists reinstates pain and precipitates cellular, somatic, and aversive signs of physical withdrawal; this phenomenon requires N-methyl-D-aspartate receptor-mediated activation of calcium-sensitive adenylyl cyclase type 1 (AC1). In this review, we present a new conceptual model of the transition from acute to chronic pain, based on the delicate balance between LS and endogenous analgesia that develops after painful tissue injury. First, injury activates pain pathways. Second, the spinal cord establishes MOR constitutive activity (MORCA) as it attempts to control pain. Third, over time, the body becomes dependent on MORCA, which paradoxically sensitizes pain pathways. Stress or injury escalates opposing inhibitory and excitatory influences on nociceptive processing as a pathological consequence of increased endogenous opioid tone. Pain begets MORCA begets pain vulnerability in a vicious cycle. The final result is a silent insidious state characterized by the escalation of two opposing excitatory and inhibitory influences on pain transmission: LS mediated by AC1 (which maintains the accelerator) and pain inhibition mediated by MORCA (which maintains the brake). This raises the prospect that opposing homeostatic interactions between MORCA analgesia and latent NMDAR-AC1-mediated pain sensitization creates a lasting vulnerability to develop chronic pain. Thus, chronic pain syndromes may result from a failure in constitutive signaling of spinal MORs and a loss of endogenous analgesic control. An overarching long-term therapeutic goal of future research is to alleviate chronic pain by either (a) facilitating endogenous opioid analgesia, thus restricting LS within a state of remission, or (b) extinguishing LS altogether.
内源性μ-阿片受体(MORs)的激活可缓解急性疼痛。最近的研究表明,组织炎症会产生潜伏性疼痛敏化(LS),这种敏化会被脊髓MOR信号掩盖数月,即使在损伤完全恢复且正常疼痛阈值重新建立之后。用MOR反向激动剂进行干扰会恢复疼痛,并引发细胞、躯体和身体戒断的厌恶症状;这种现象需要N-甲基-D-天冬氨酸受体介导的1型钙敏腺苷酸环化酶(AC1)的激活。在这篇综述中,我们基于疼痛性组织损伤后发展起来的LS与内源性镇痛之间的微妙平衡,提出了一个从急性疼痛转变为慢性疼痛的新概念模型。首先,损伤激活疼痛通路。其次,脊髓在试图控制疼痛时建立MOR组成性活性(MORCA)。第三,随着时间的推移,身体会依赖于MORCA,而这自相矛盾地使疼痛通路敏感化。作为内源性阿片类物质张力增加的病理后果,压力或损伤会加剧对伤害性处理的相反抑制性和兴奋性影响。疼痛引发MORCA,进而导致疼痛易感性,形成恶性循环。最终结果是一种隐匿的无声状态,其特征是对疼痛传递的两种相反的兴奋性和抑制性影响不断升级:由AC1介导的LS(维持加速器)和由MORCA介导的疼痛抑制(维持制动器)。这就提出了一种可能性,即MORCA镇痛与潜伏性NMDAR-AC1介导的疼痛敏化之间相反的稳态相互作用会造成产生慢性疼痛的持久易感性。因此,慢性疼痛综合征可能是由于脊髓MORs的组成性信号传导失败和内源性镇痛控制丧失所致。未来研究的一个总体长期治疗目标是通过以下两种方式缓解慢性疼痛:(a)促进内源性阿片类物质镇痛,从而将LS限制在缓解状态,或(b)完全消除LS。