Nazir Sheraz A, Khan Jamal N, Mahmoud Islam Z, Greenwood John P, Blackman Daniel J, Kunadian Vijay, Been Martin, Abrams Keith R, Wilcox Robert, Adgey A A Jennifer, McCann Gerry P, Gershlick Anthony H
Department of Cardiovascular Sciences, University of Leicester and the NIHR Leicester Cardiovascular Biomedical Research Unit, Glenfield Hospital, Groby Road, LE3 9QP Leicester, UK.
Trials. 2014 Sep 25;15:371. doi: 10.1186/1745-6215-15-371.
Microvascular obstruction (MVO) secondary to ischaemic-reperfusion injury is an important but underappreciated determinant of short- and longer-term outcome following percutaneous coronary intervention (PCI) treatment of ST-elevation myocardial infarction (STEMI). Several small studies have demonstrated a reduction in the degree of MVO utilising a variety of vasoactive agents, with adenosine and sodium nitroprusside (SNP) being most evaluated. However, the evidence base remains weak as the trials have had variable endpoints, differing drug doses and delivery. As such, the results regarding benefit are conflicting.
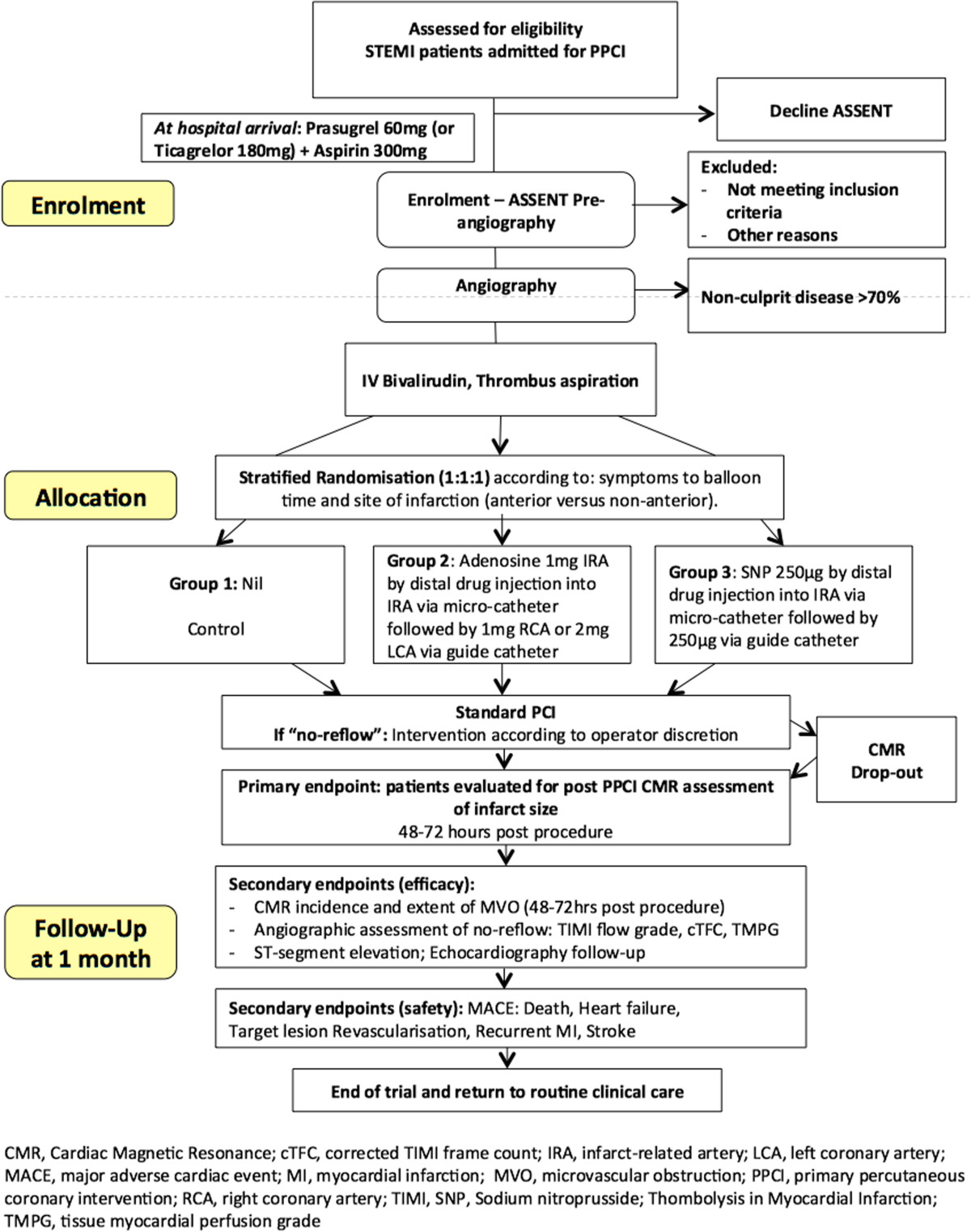
The REperfusion Facilitated by LOcal adjunctive therapy in STEMI (REFLO-STEMI) trial is a multicentre, prospective, randomised, controlled, open label, study with blinded endpoint analysis: Patients presenting within 6 h of onset of STEMI and undergoing planned primary PCI (P-PCI) with TIMI 0/1 flow in the infarct-related artery (IRA) and no significant bystander coronary artery disease on angiography, are randomised into one of three groups: PCI with adjunctive pharmacotherapy (intracoronary adenosine or SNP) or control (standard PCI). All receive Bivalirudin anticoagulation and thrombus aspiration. The primary outcome is infarct size (IS) (determined as a percentage of total left ventricular mass) measured by cardiac magnetic resonance imaging (CMRI) undertaken at 48 to 72 h post P-PCI. Secondary outcome measures include MVO (hypoenhancement within infarct core) on CMRI, angiographic markers of microvascular perfusion and MACE during 1-month follow-up. The study aims to recruit 240 patients (powered at 80% to detect a 5% absolute reduction in IS).
The REFLO-STEMI study has been designed to address the weaknesses of previous trials, which have collectively failed to demonstrate whether adjunctive pharmacotherapy with adenosine and/or SNP can reduce measures of myocardial injury (infarct size and MVO) and improve clinical outcome, despite good basic evidence that they have the potential to attenuate this process. The REFLO-STEMI study will be the most scientifically robust trial to date evaluating whether adjunctive therapy (intracoronary adenosine or SNP following thrombus aspiration) reduces CMRI measured IS and MVO in patients undergoing P-PCI within 6 h of onset of STEMI.
Trial registered 20th November 2012: ClinicalTrials.gov Identifier NCT01747174.
缺血再灌注损伤继发的微血管阻塞(MVO)是ST段抬高型心肌梗死(STEMI)经皮冠状动脉介入治疗(PCI)后短期和长期预后的一个重要但未得到充分认识的决定因素。几项小型研究表明,使用多种血管活性药物可降低MVO的程度,其中腺苷和硝普钠(SNP)得到的评估最多。然而,由于试验的终点不同、药物剂量和给药方式各异,证据基础仍然薄弱。因此,关于获益的结果相互矛盾。
STEMI局部辅助治疗促进再灌注(REFLO-STEMI)试验是一项多中心、前瞻性、随机、对照、开放标签、终点分析设盲的研究:STEMI发病6小时内就诊且计划进行直接PCI(P-PCI),梗死相关动脉(IRA)TIMI血流0/1级且血管造影显示无明显的非梗死相关冠状动脉疾病的患者,被随机分为三组之一:PCI联合辅助药物治疗(冠状动脉内注射腺苷或SNP)或对照组(标准PCI)。所有患者均接受比伐卢定抗凝和血栓抽吸。主要结局是P-PCI后48至72小时通过心脏磁共振成像(CMRI)测量的梗死面积(IS)(以左心室总质量的百分比表示)。次要结局指标包括CMRI上的MVO(梗死核心内强化减弱)、微血管灌注的血管造影标记物以及1个月随访期间的主要不良心血管事件(MACE)。该研究旨在招募240名患者(检验效能为80%,以检测IS绝对降低5%)。
REFLO-STEMI研究旨在解决以往试验的不足之处,尽管有充分的基础证据表明腺苷和/或SNP有可能减轻这一过程,但以往试验总体上未能证明辅助药物治疗能否减少心肌损伤指标(梗死面积和MVO)并改善临床结局。REFLO-STEMI研究将是迄今为止最具科学性的试验,评估辅助治疗(血栓抽吸后冠状动脉内注射腺苷或SNP)是否能减少STEMI发病6小时内接受P-PCI患者CMRI测量的IS和MVO。
2012年11月20日注册:ClinicalTrials.gov标识符NCT01747174。