Kim Jong Man, Cho Wontae, Kwon Choon Hyuck David, Joh Jae-Won, Park Jae Berm, Ko Justin Sangwook, Gwak Mi Sook, Kim Gaab Soo, Kim Sung Joo, Lee Suk-Koo
Department of Surgery, Samsung Medical Center (JMK, WC, CHDK, J-WJ, JBP, SJK, SKL); and Department of Anesthesiology and Pain Medicine (JSK, MSG, GSK), Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Medicine (Baltimore). 2014 Sep;93(14):e84. doi: 10.1097/MD.0000000000000084.
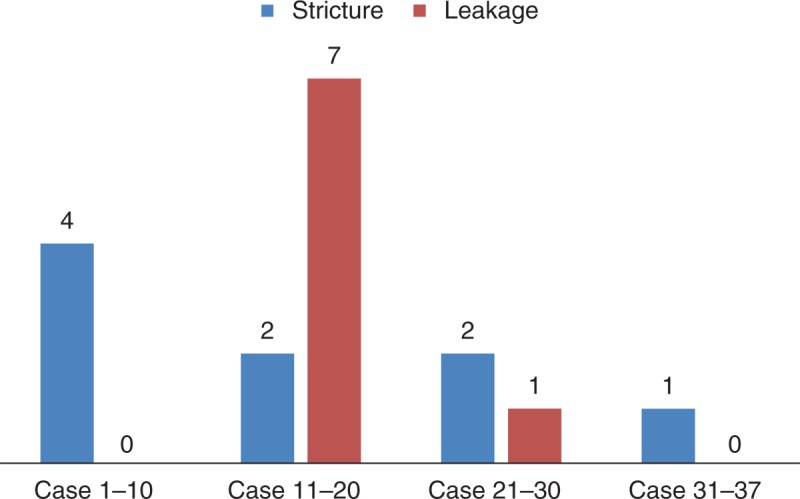
Biliary strictures and bile leaks account for the majority of biliary complications after living donor liver transplantation (LDLT). The aim of this study was to examine differences in biliary complications after adult LDLTs were performed by an experienced senior surgeon and an inexperienced junior surgeon. Surgeries included bile duct reconstruction after adult LDLT using a right liver graft, and risk factors for biliary stricture were identified. We retrospectively reviewed the medical records of 136 patients who underwent LDLT in order to identify patients who developed biliary complications. The senior surgeon performed 102 surgeries and the junior surgeon performed 34 surgeries. The proportion of patients with biliary stricture was similar between the senior and the junior surgeons (27.5% vs 26.5%; P = 0.911). However, the incidence of biliary leakage was higher in patients of the junior surgeon than in those of the senior surgeon (23.5% vs 2.9%; P = 0.001). The frequency of percutaneous drainage was also higher for the junior surgeon than the senior surgeon because of the junior surgeon's high leakage rate of the drainage. When the junior surgeon performed bile duct anastomosis, biliary leakage occurred in 7 patients between the 11th and 20th cases. However, biliary leakage occurred in only 1 case thereafter. Bile duct reconstruction performed by beginner surgeons in LDLT using right lobe grafts should be cautiously monitored and observed by a senior surgeon until an inexperienced junior surgeon has performed at least 20 cases, because of the high incidence of biliary leakage related to surgeon's inexperience in bile duct reconstructions in LDLT.
胆管狭窄和胆漏是活体肝移植(LDLT)后胆道并发症的主要类型。本研究旨在探讨由经验丰富的资深外科医生和经验不足的初级外科医生进行成人LDLT术后胆道并发症的差异。手术包括使用右肝移植物进行成人LDLT后的胆管重建,并确定胆管狭窄的危险因素。我们回顾性分析了136例行LDLT患者的病历,以确定发生胆道并发症的患者。资深外科医生进行了102例手术,初级外科医生进行了34例手术。资深外科医生和初级外科医生的胆管狭窄患者比例相似(27.5%对26.5%;P = 0.911)。然而,初级外科医生组患者的胆漏发生率高于资深外科医生组(23.5%对2.9%;P = 0.001)。由于初级外科医生引流的高漏率,其经皮引流的频率也高于资深外科医生。当初级外科医生进行胆管吻合时,第11至20例中有7例发生胆漏。然而,此后仅1例发生胆漏。在LDLT中使用右叶移植物进行胆管重建时,由于初级外科医生在LDLT胆管重建中缺乏经验导致胆漏发生率较高,因此在经验不足的初级外科医生至少完成20例手术之前,应由资深外科医生谨慎监测和观察。