Prachayakul Varayu, Aswakul Pitulak, Bhunthumkomol Patommatat, Deesomsak Morakod
Department of Internal Medicine, Siriraj GI Endoscopy Center, Siriraj Hospital, Division of Gastroenterology, Faculty of Medicine, Mahidol University, Bangkok, Thailand.
BMC Gastroenterol. 2014 Sep 26;14:165. doi: 10.1186/1471-230X-14-165.
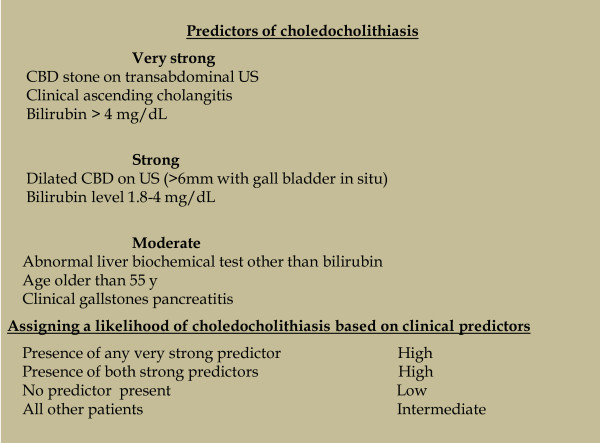
Diagnosis of choledocholithiasis requires clinical manifestations and imaging examination findings suggesting a stone in the common bile duct (CBD), but these factors are not highly sensitive or specific. The choledocholithiasis management algorithm proposed by the American Society for Gastrointestinal Endoscopy (ASGE) may not be appropriate for patients who fulfill the clinical criteria for a high likelihood of choledocholithiasis. Endoscopic ultrasonography (EUS) may replace endoscopic retrograde cholangiopancreatography (ERCP) for the detection of CBD stones in all patients. The aims of this study were to determine the diagnostic yield and optimal timing of EUS in patients with an intermediate or high likelihood of choledocholithiasis requiring therapeutic ERCP.
Patients with suspected choledocholithiasis who underwent EUS between June 2009 and January 2012 were retrospectively reviewed. The patients were divided into two groups based on the likelihood of choledocholithiasis according to the clinical predictors described by the ASGE guidelines: an intermediate likelihood group and a high likelihood group. The demographic data, clinical manifestations at presentation, blood test results, EUS and ERCP findings, and clinical manifestations during the follow-up period were recorded and analyzed.
Ninety-three patients were enrolled in the study (52.7% in the intermediate likelihood group and 47.3% in the high likelihood group). CBD stones were detected in 22.44% of patients in the intermediate likelihood group and 38.63% of patients in the high likelihood group. EUS had a sensitivity of 100% and specificity of 80% for detection of CBD stones. An alkaline phosphatase level of > 133 mg/dL (area under the curve, 0.576) was the only factor that was significantly associated with detection of CBD stones in patients who underwent EUS > 7 days after the initial clinical presentation (odds ratio 4.87, p = 0.01).
EUS is an accurate diagnostic tool for the detection of CBD stones, and can prevent the unnecessary use of ERCP. This study found that use of clinical criteria alone might not provide a good prediction of the presence of CBD stones, even in patients who fulfill the criteria for a high likelihood of choledocholithiasis.
胆总管结石的诊断需要临床表现和影像学检查结果提示胆总管(CBD)存在结石,但这些因素的敏感性和特异性都不高。美国胃肠内镜学会(ASGE)提出的胆总管结石处理算法可能不适用于符合胆总管结石高度可能性临床标准的患者。内镜超声检查(EUS)可能取代内镜逆行胰胆管造影(ERCP)用于所有患者胆总管结石的检测。本研究的目的是确定在需要治疗性ERCP的胆总管结石可能性为中度或高度的患者中,EUS的诊断率及最佳时机。
对2009年6月至2012年1月期间接受EUS检查的疑似胆总管结石患者进行回顾性研究。根据ASGE指南中描述的临床预测指标,将患者按胆总管结石可能性分为两组:中度可能性组和高度可能性组。记录并分析患者的人口统计学数据、就诊时的临床表现、血液检查结果、EUS和ERCP检查结果以及随访期间的临床表现。
93例患者纳入研究(中度可能性组占52.7%,高度可能性组占47.3%)。中度可能性组22.44%的患者和高度可能性组38.63%的患者检测到胆总管结石。EUS检测胆总管结石的敏感性为100%,特异性为80%。碱性磷酸酶水平>133 mg/dL(曲线下面积,0.576)是在初次临床表现>7天后接受EUS检查的患者中与检测到胆总管结石显著相关的唯一因素(比值比4.87,p = 0.01)。
EUS是检测胆总管结石的准确诊断工具,可避免不必要的ERCP使用。本研究发现,仅使用临床标准可能无法很好地预测胆总管结石的存在,即使是符合胆总管结石高度可能性标准的患者。