Huang Chang-Ming, Zhang Jun-Rong, Zheng Chao-Hui, Li Ping, Xie Jian-Wei, Wang Jia-Bin, Lin Jian-Xian, Lu Jun, Chen Qi-Yue
Department of Gastric Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian Province, China.
PLoS One. 2014 Sep 29;9(9):e108480. doi: 10.1371/journal.pone.0108480. eCollection 2014.
This study was designed to formulate a model that efficiently predicts splenic hilar lymph node metastasis (SHLNM) in patients with proximal gastric cancer and to assess indications for laparoscopic spleen-preserving no.10 lymph node dissection (LSPNo.10LND) based on this model.
Patients (N = 346) with proximal gastric cancer who underwent LSPNo.10LND from January 2010 to October 2013 were prospectively enrolled and retrospectively evaluated. Groups of patients with and without SHLNM were compared, and independent risk factors for SHLNM determined. An optimal predictive model of SHLNM in patients with proximal gastric cancer was well established.
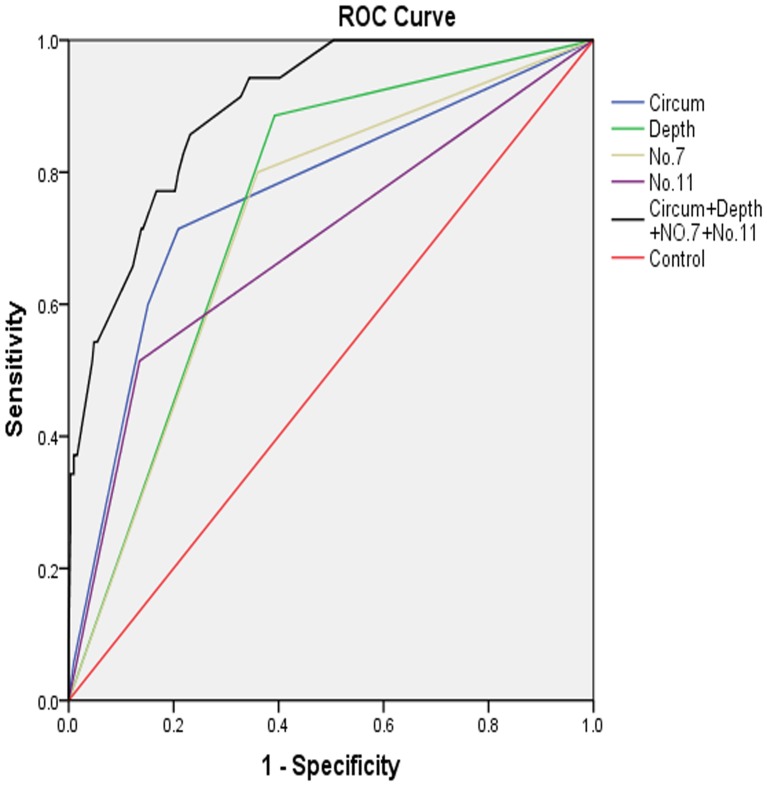
Of the 346 patients with proximal gastric cancer, only 35 (10.1%) were diagnosed with SHLNM. Depth of invasion, tumor location and metastases to No.7 and No.11 lymph nodes (LNs) were independent risk factors for SHLNM (p<0.0001 each). A model involving depth of invasion, tumor location and metastasis to No.7 and 11 LNs yielded a lowest Akaike's information criterion (AIC) of -913.535 and a highest area under the ROC curve (AUC) of 0.897(95%CI:0.851-0.944). Stratification analysis showed no SHLNMs in the absence of serosal invasion of the lesser curvature and metastases at No.7 and No.11 LNs (T2-3∶0/87, 95% CI: 0.00-4.15).
A model including depth of invasion, tumor location and metastases at No.7 and No.11 LNs was found optimal for predicting SHLNM for proximal gastric cancers. LSPNo.10LND may be avoided when tumors on the lesser curvature did not show serosal invasion or metastases at No.7 and No.11 LNs.
本研究旨在构建一个能有效预测近端胃癌患者脾门淋巴结转移(SHLNM)的模型,并基于该模型评估腹腔镜保脾第10组淋巴结清扫术(LSPNo.10LND)的适应证。
前瞻性纳入2010年1月至2013年10月期间接受LSPNo.10LND的近端胃癌患者(N = 346例),并进行回顾性评估。比较有和无SHLNM的患者组,确定SHLNM的独立危险因素。建立了近端胃癌患者SHLNM的最佳预测模型。
346例近端胃癌患者中,仅35例(10.1%)被诊断为SHLNM。浸润深度、肿瘤位置以及第7组和第11组淋巴结转移是SHLNM的独立危险因素(各p<0.0001)。一个包含浸润深度、肿瘤位置以及第7组和第11组淋巴结转移的模型产生了最低的赤池信息准则(AIC)-913.535和最高的ROC曲线下面积(AUC)0.897(95%CI:0.851 - 0.944)。分层分析显示,在小弯侧无浆膜侵犯且第7组和第11组淋巴结无转移的情况下无SHLNM(T2 - 3∶0/87,95%CI:0.00 - 4.15)。
发现一个包含浸润深度、肿瘤位置以及第7组和第11组淋巴结转移的模型最适合预测近端胃癌的SHLNM。当小弯侧肿瘤未显示浆膜侵犯或第7组和第11组淋巴结无转移时,可避免行LSPNo.10LND。