Little Virginia L, McGuirk Theresa E, Patten Carolynn
Department of Physical Therapy, University of Florida, Gainesville, FL, United States of America; Rehabilitation Science Doctoral Program, University of Florida, Gainesville, FL, United States of America; Brain Rehabilitation Research & Development Center, Malcolm-Randall VA Medical Center, Gainesville, FL, United States of America.
Department of Physical Therapy, University of Florida, Gainesville, FL, United States of America; Brain Rehabilitation Research & Development Center, Malcolm-Randall VA Medical Center, Gainesville, FL, United States of America.
PLoS One. 2014 Oct 16;9(10):e110140. doi: 10.1371/journal.pone.0110140. eCollection 2014.
Difficulty advancing the paretic limb during the swing phase of gait is a prominent manifestation of walking dysfunction following stroke. This clinically observable sign, frequently referred to as 'foot drop', ostensibly results from dorsiflexor weakness.
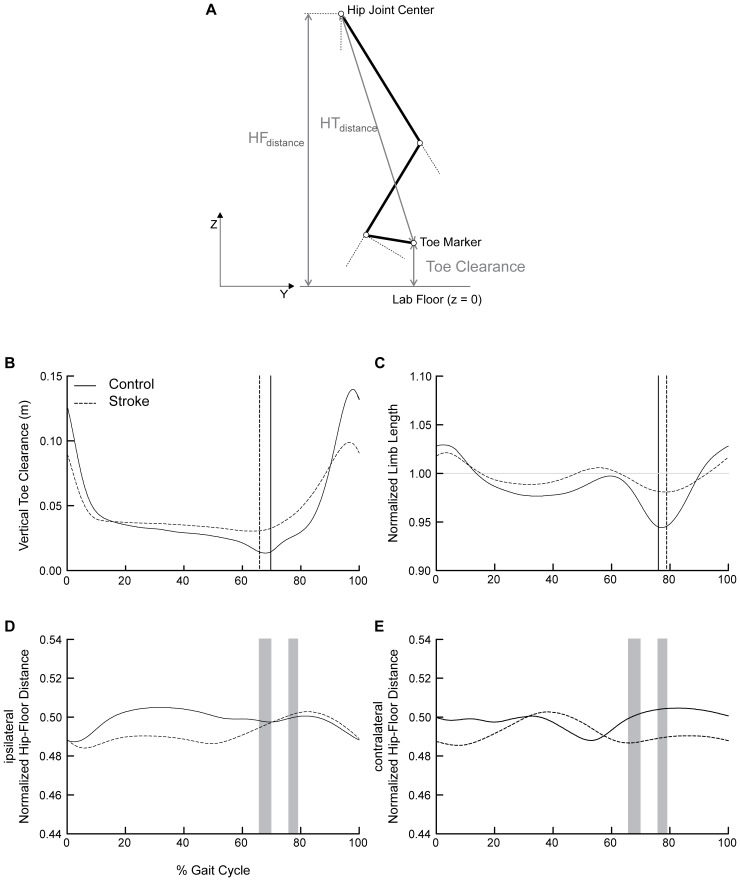
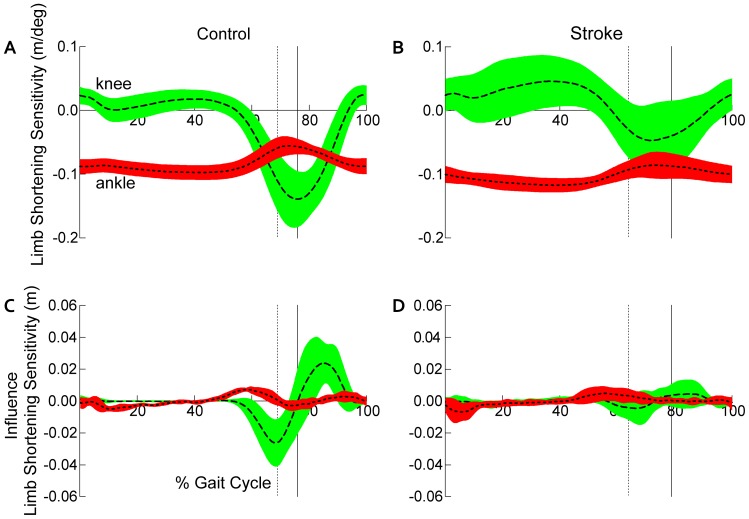
Here we investigated the extent to which hip, knee, and ankle motions contribute to impaired paretic limb advancement. We hypothesized that neither: 1) minimal toe clearance and maximal limb shortening during swing nor, 2) the pattern of multiple joint contributions to toe clearance and limb shortening would differ between post-stroke and non-disabled control groups.
We studied 16 individuals post-stroke during overground walking at self-selected speed and nine non-disabled controls who walked at matched speeds using 3D motion analysis.
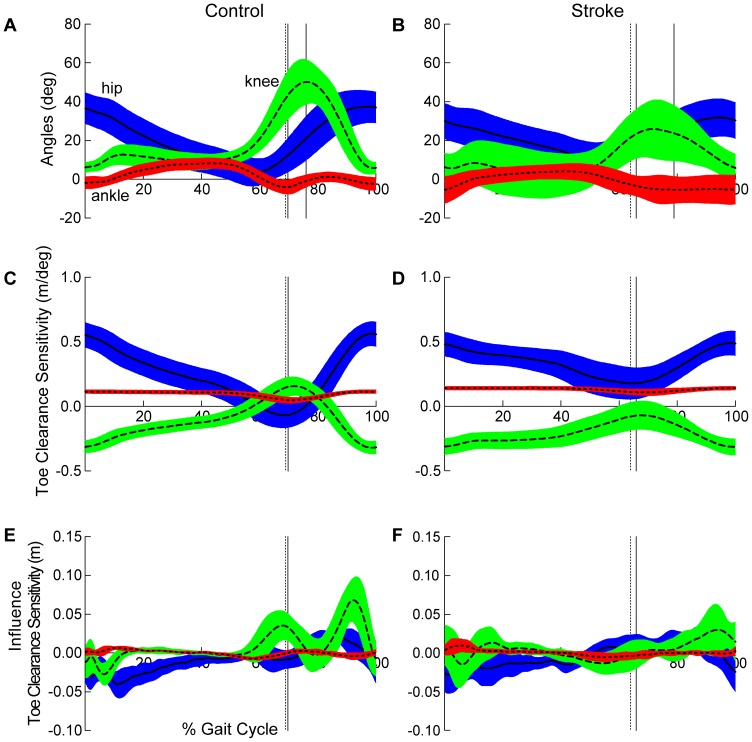
No differences were detected with respect to the ankle dorsiflexion contribution to toe clearance post-stroke. Rather, hip flexion had a greater relative influence, while the knee flexion influence on producing toe clearance was reduced.
Similarity in the ankle dorsiflexion, but differences in the hip and knee, contributions to toe clearance between groups argues strongly against dorsiflexion dysfunction as the fundamental impairment of limb advancement post-stroke. Marked reversal in the roles of hip and knee flexion indicates disruption of inter-joint coordination, which most likely results from impairment of the dynamic contribution to knee flexion by the gastrocnemius muscle in preparation for swing. These findings suggest the need to reconsider the notion of foot drop in persons post-stroke. Redirecting the focus of rehabilitation and restoration of hemiparetic walking dysfunction appropriately, towards contributory neuromechanical impairments, will improve outcomes and reduce disability.
在步态摆动期患侧肢体推进困难是中风后行走功能障碍的一个突出表现。这种临床上可观察到的体征,常被称为“足下垂”,表面上是由背屈肌无力导致的。
在此,我们研究了髋、膝和踝关节运动在多大程度上导致患侧肢体推进受损。我们假设:1)摆动期最小足趾间隙和最大肢体缩短,以及2)多关节对足趾间隙和肢体缩短的贡献模式,在中风后组和非残疾对照组之间没有差异。
我们使用三维运动分析研究了16名中风后个体以自选速度在地面行走的情况,以及9名非残疾对照组以匹配速度行走的情况。
在中风后,未检测到踝关节背屈对足趾间隙贡献的差异。相反,髋关节屈曲的相对影响更大,而膝关节屈曲对产生足趾间隙的影响减小。
两组之间踝关节背屈对足趾间隙贡献的相似性,以及髋、膝关节贡献的差异,有力地反驳了背屈功能障碍是中风后患侧肢体推进基本损伤的观点。髋、膝关节屈曲作用的明显逆转表明关节间协调受到破坏,这很可能是由于腓肠肌对膝关节屈曲的动态贡献在摆动准备阶段受损所致。这些发现表明有必要重新考虑中风患者足下垂的概念。将偏瘫步行功能障碍康复和恢复的重点适当地转向相关的神经机械损伤,将改善治疗效果并减少残疾。