Parpia Sameer, Julian Jim A, Thabane Lehana, Gu Chushu, Whelan Timothy J, Levine Mark N
Ontario Clinical Oncology Group, Department of Oncology, McMaster University, Hamilton, Ontario, Canada.
Centre of Evaluation of Medicines, St Joseph's Hospital, Hamilton, Ontario, Canada.
BMJ Open. 2014 Oct 24;4(10):e006531. doi: 10.1136/bmjopen-2014-006531.
In non-inferiority trials of radiotherapy in patients with early stage breast cancer, it is inevitable that some patients will cross over from the experimental arm to the standard arm prior to initiation of any treatment due to complexities in treatment planning or subject preference. Although the intention-to-treat (ITT) analysis is the preferred approach for superiority trials, its role in non-inferiority trials is still under debate. This has led to the use of alternative approaches such as the per-protocol (PP) analysis or the as-treated (AT) analysis, despite the inherent biases of such approaches.
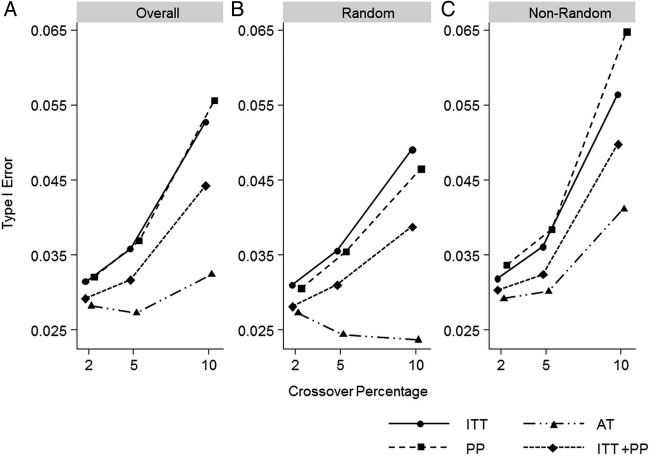
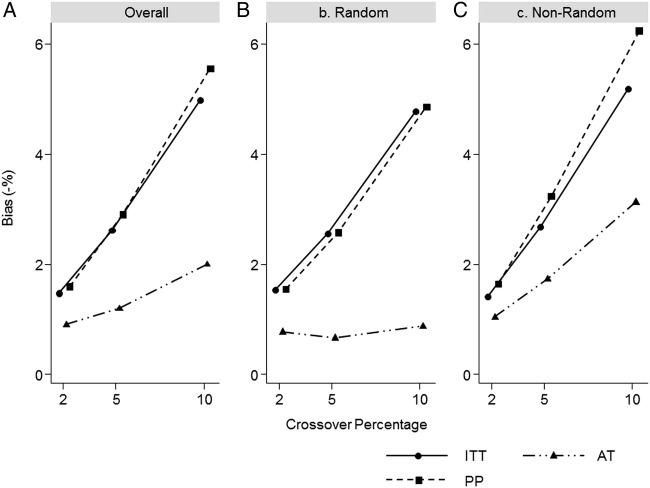
Using simulations, we investigate the effect of 2%, 5% and 10% random and non-random crossovers prior to radiotherapy initiation on the ITT, PP, AT and the combination of ITT and PP analyses with respect to type I error in trials with time-to-event outcomes. We also evaluate bias and SE of the estimates from the ITT, PP and AT approaches.
The AT approach had the best performance in terms of type I error, but was anticonservative as non-random crossover increased. The ITT and PP approaches were anticonservative under all percentages of random and non-random crossover. Similarly, lowest bias was seen with the AT approach; however, bias increased as the percentage of non-random crossover increased. The ITT and PP had poor performance in terms of bias as crossovers increased.
If minimal crossovers were to occur, we have shown that the AT approach has the lowest type I error rates and smallest opportunity for bias. Results of trials with a high number of crossovers should be interpreted with caution, especially when crossover is non-random. Attempts to prevent crossovers should be maximised.
在早期乳腺癌患者放疗的非劣效性试验中,由于治疗计划的复杂性或受试者偏好,不可避免地会有一些患者在开始任何治疗之前从试验组转至标准组。尽管意向性分析(ITT)是优效性试验的首选方法,但其在非劣效性试验中的作用仍存在争议。这导致了替代方法的使用,如符合方案分析(PP)或实际治疗分析(AT),尽管这些方法存在固有偏差。
通过模拟,我们研究了在放疗开始前2%、5%和10%的随机和非随机交叉对ITT、PP、AT以及ITT和PP分析相结合在具有事件发生时间结局的试验中I型错误的影响。我们还评估了ITT、PP和AT方法估计值的偏差和标准误。
就I型错误而言,AT方法表现最佳,但随着非随机交叉的增加,它是反保守的。在所有随机和非随机交叉百分比下,ITT和PP方法都是反保守的。同样,AT方法的偏差最低;然而,随着非随机交叉百分比的增加,偏差也会增加。随着交叉的增加,ITT和PP在偏差方面表现不佳。
如果发生的交叉最少,我们已经表明AT方法具有最低的I型错误率和最小的偏差机会。对交叉数量较多的试验结果应谨慎解释,尤其是当交叉是非随机的时候。应最大限度地尝试防止交叉。