Boersma Doeke, van Eekeren Ramon R J P, Kelder Hans J C, Werson Debora A B, Holewijn Suzanne, Schreve Michiel A, Reijnen Michel M P J, de Vries Jean Paul P M
Department of Vascular Surgery, St Antonius Hospital, Koekoeklaan 1, 3435 CM Nieuwegein, The Netherlands.
Trials. 2014 Oct 29;15:421. doi: 10.1186/1745-6215-15-421.
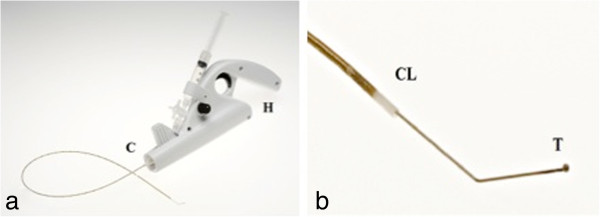
Minimally invasive endothermal techniques, for example, radiofrequency ablation (RFA), have revolutionized the treatment of insufficient truncal veins and are associated with an excellent outcome. The use of thermal energy requires the instillation of tumescent anesthesia around the vein. Mechanochemical endovenous ablation (MOCA™) combines mechanical endothelial damage, using a rotating wire, with simultaneous infusion of a liquid sclerosans. Tumescent anesthesia is not required as no heat is used. Prospective studies using MOCA™ in both great and small saphenous veins showed good anatomical and clinical results with fast postoperative recovery.
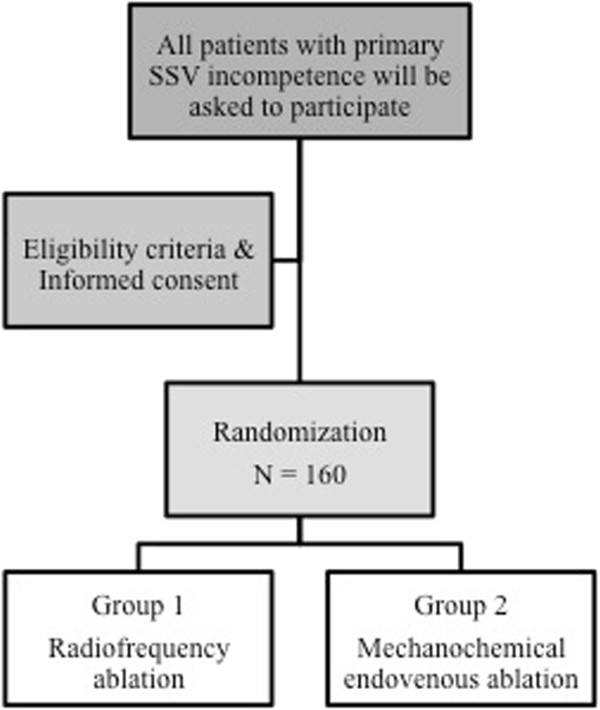
METHODS/DESIGN: The MESSI trial (Mechanochemical Endovenous ablation versus radiofrequency ablation in the treatment of primary Small Saphenous vein Insufficiency) is a multicenter randomized controlled trial in which a total of 160 patients will be randomized (1:1) to MOCA™ or RFA. Consecutive patients with primary small saphenous vein incompetence, who meet the eligibility criteria, will be invited to participate in this trial. The primary endpoint is anatomic success, defined as occlusion of the treated veins objectified with duplex ultrasonography at 1 year follow-up. Secondary endpoints are post-procedural pain, initial technical success, clinical success, complications and the duration of the procedure. Initial technical success is defined as the ability to position the device adequately, treat the veins as planned and occlude the treated vein directly after the procedure has been proven by duplex ultrasonography. Clinical success is defined as an objective improvement of clinical outcome after treatment, measured with the Venous Clinical Severity Score (VCSS). Power analyses are conducted for anatomical success and post-procedural pain.Both groups will be evaluated on an intention-to-treat principle.
The hypothesis of the MESSI trial is that the anatomic success rate of MOCA™ is not inferior to RFA. The second hypothesis is that post-procedural pain is significantly less after MOCA compared to RFA.
NTR4613 Date of trial registration: 28 May 2014.
微创内热技术,例如射频消融术(RFA),彻底改变了对下肢主干静脉功能不全的治疗方式,且疗效显著。使用热能需要在静脉周围注入肿胀麻醉剂。机械化学性静脉内消融术(MOCA™)将使用旋转导丝造成的机械性内皮损伤与同时注入液体硬化剂相结合。由于不使用热能,因此无需肿胀麻醉。在大隐静脉和小隐静脉中使用MOCA™的前瞻性研究显示,术后恢复快,解剖学和临床效果良好。
方法/设计:MESSI试验(机械化学性静脉内消融术与射频消融术治疗原发性小隐静脉功能不全的对比研究)是一项多中心随机对照试验,共160例患者将按1:1随机分为接受MOCA™或RFA治疗。符合入选标准的原发性小隐静脉功能不全的连续患者将被邀请参加本试验。主要终点是解剖学成功,定义为在1年随访时通过双功超声检查证实治疗的静脉闭塞。次要终点包括术后疼痛、初始技术成功、临床成功、并发症和手术持续时间。初始技术成功定义为能够充分放置设备,按计划治疗静脉,并在手术后通过双功超声检查证实治疗的静脉闭塞。临床成功定义为治疗后临床结局的客观改善,采用静脉临床严重程度评分(VCSS)进行测量。对解剖学成功和术后疼痛进行功效分析。两组均按照意向性分析原则进行评估。
MESSI试验的假设是,MOCA™的解剖学成功率不低于RFA。第二个假设是,与RFA相比,MOCA术后疼痛明显减轻。
NTR4613 试验注册日期:2014年5月28日。