Samarawickrama Amanda, Jose Sophie, Sabin Caroline, Walker-Bone Karen, Fisher Martin, Gilleece Yvonne
Clinical Investigation and Research Unit, Brighton and Sussex Medical School, Brighton, UK.
Department of Infection and Population Health, University College London, London, UK.
J Int AIDS Soc. 2014 Nov 2;17(4 Suppl 3):19568. doi: 10.7448/IAS.17.4.19568. eCollection 2014.
Combination antiretroviral therapy (cART) may affect vitamin D [25(OH)D], parathyroid hormone (PTH), bone mineral density (BMD) and bone turnover (BT). Reduced BMD and secondary hyperparathyroidism have been reported with tenofovir (TDF). We investigated the associations between TDF and bone markers, especially in 25(OH)D-deficient patients.
In a single-centre longitudinal study investigating BMD in HIV-positive men, serum 25(OH)D, calcium, phosphate, PTH and alkaline phosphatase (ALP) were measured. Lumbar spine, non-dominant total hip and non-dominant femoral neck BMD (g/cm(2)) were measured using dual-energy X-ray absorptiometry. BT was assessed by serum type 1 procollagen (P1NP) and carboxy-terminal collagen cross-links (CTX). Mann-Whitney U tests compared serum markers and BT, and t-tests compared BMD according to TDF in all and 25(OH)D-deficient patients.
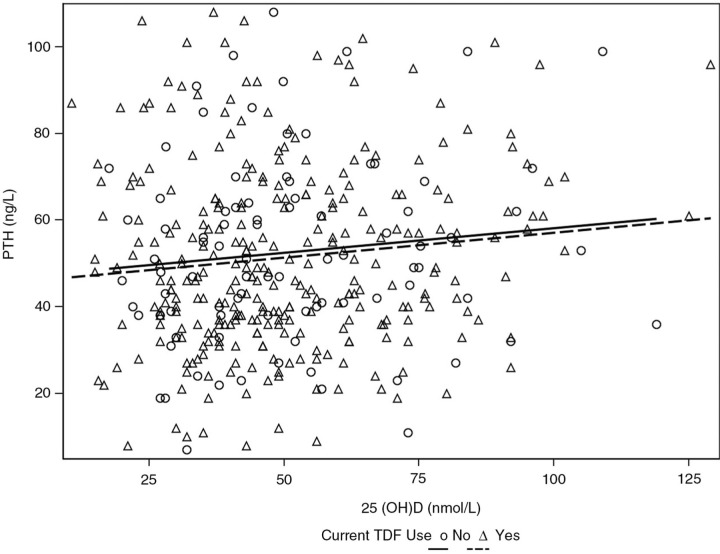
A total of 422 men were recruited: mean age 47 (SD 9.8) years, 94% white ethnicity, 93% MSM, diagnosed HIV positive for median 9.6 (IQR 5.0,15.5) years, median CD4 547 (IQR 411,696) cells/µL, HIV RNA <40 copies/mL in 87% (96% of those on cART). 25(OH)D (nmol/L) was normal (>75), insufficient (50-75), deficient (25-50) and severely deficient (<25) in 14%, 29%, 50% and 7%, respectively. Of 381 men on cART, 77% were currently on TDF. TDF was not associated with median calcium (p=0.69) or phosphate (p=0.52), but patients had higher (but normal) median ALP [81 (IQR 69,103) vs. 73 (IQR 60,89) IU/L, p=0.005) compared to non-TDF cART. There was no difference in the association between vitamin D and PTH according to whether someone currently was (r=0.11, p=0.06, Figure 1) or was not using TDF (r=0.12, p=0.29, Figure 1). TDF was also not associated with PTH, BMD or BT in either all patients on cART (Table 1a) or in patients with 25(OH)D deficiency (Table 1b).
In this largely TDF-experienced cohort of HIV-positive men, there was no association between TDF and 25(OH)D deficiency, hyperparathyroidism, reduced BMD or increased BT, although patients on TDF had higher but normal ALP. We found no evidence to support additional monitoring of bone markers in patients on TDF regardless of 25(OH)D status.
联合抗逆转录病毒疗法(cART)可能会影响维生素D [25(OH)D]、甲状旁腺激素(PTH)、骨矿物质密度(BMD)和骨转换(BT)。据报道,替诺福韦(TDF)会导致骨密度降低和继发性甲状旁腺功能亢进。我们研究了TDF与骨标志物之间的关联,尤其是在25(OH)D缺乏的患者中。
在一项调查HIV阳性男性骨密度的单中心纵向研究中,测量了血清25(OH)D、钙、磷、PTH和碱性磷酸酶(ALP)。使用双能X线吸收法测量腰椎、非优势侧全髋关节和非优势侧股骨颈的骨密度(g/cm²)。通过血清I型前胶原(P1NP)和羧基末端胶原交联(CTX)评估骨转换。Mann-Whitney U检验比较血清标志物和骨转换,t检验根据是否使用TDF比较所有患者和25(OH)D缺乏患者的骨密度。
共招募了422名男性:平均年龄47(标准差9.8)岁,94%为白人,93%为男男性行为者,确诊HIV阳性的中位时间为9.6(四分位间距5.0,15.5)年,中位CD4为547(四分位间距411,696)个细胞/µL,87%的患者HIV RNA <40拷贝/mL(接受cART治疗的患者中96%达到此水平)。25(OH)D(nmol/L)正常(>75)、不足(50 - 75)、缺乏(25 - 50)和严重缺乏(<25)的患者分别占14%、29%、50%和7%。在381名接受cART治疗的男性中