Pinnetti Carmela, Lorenzini Patrizia, Cozzi-Lepri Alessandro, Sandrine Ottou, Tommasi Chiara, Zaccarelli Mauro, Perno Carlo Federico, Capobianchi Maria Rosaria, Girardi Enrico, Antinori Andrea, Ammassari Adriana
Clinical Department, National Institute for Infectious Diseases Lazzaro Spallanzani IRCCS, Roma, Italy.
Research Department of Infection and Population Health, University College, London, UK.
J Int AIDS Soc. 2014 Nov 2;17(4 Suppl 3):19809. doi: 10.7448/IAS.17.4.19809. eCollection 2014.
PI/r monotherapy has been suggested as an attainable maintenance strategy in patients achieving stable HIV suppression in plasma. The objective of trial was to compare the virological outcome of two different PI/r QD monotherapy strategies (LPV/r or DRV/r) with maintaining a triple PI/r-based ARV regimen.
Phase III, open-label, non-inferiority (-12% margin), randomized trial of HIV adults with HIV-RNA <50 cp/mL for at least 48 weeks while on PI/r-based cART, CD4 nadir >100 cell/mm(3), without previous PIs virological failure. Eligible patients were randomized to continue PI/r+2NRTIs (Arm A), to switch to LPV/r 800/200 mg QD monotherapy (Arm B), or to switch to DRV/r 800/100 mg QD monotherapy (Arm C). Primary endpoint was proportion of patients with plasma HIV-1 RNA <50 cp/mL (TLOVR) at 48w by intent to treat (ITT) analysis (missing/re-induction=failure). FDA snapshot and ITT switch-included analysis (ITT-SI) were also used. In ITT-SI, patients who had <50 copies/mL at 96w were counted as successes even if they had confirmed HIV-RNA elevations and had subsequently successfully intensified by NRTI.
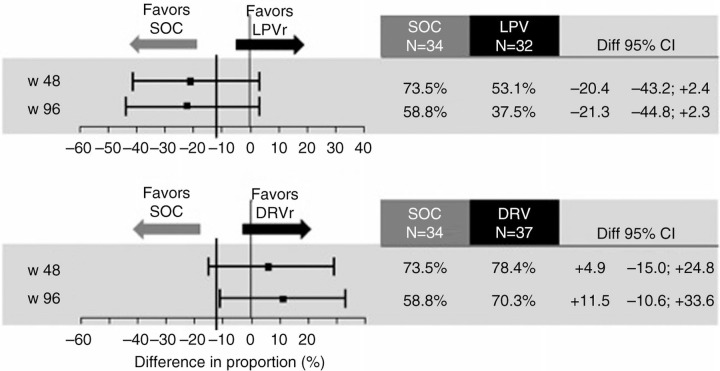
Due to slow recruitment, only 103 patients were included. No differences were observed between the three arms with respect to gender, age, HIV transmission, CD4 nadir and at screening. At randomization, 61 patients were receiving TDF/FTC (60%), 19 ZDV/3TC (18%), 8 ABV/3TC (8%), 75 LPV/r (73%), 13 ATV/r (13%), 4 DRV/r (4%). Differences in proportion of virological success by groups using Arm A as comparator according to FDA TLOVR were reported in Figure 1. Similar results were obtained by Snapshot analysis. Of 14 patients with virological failure, 8 patients restarted triple therapy with 2NRTI and 7/8 regained a VL <50 cp/mL over time. According to ITT-SI analysis, 96 week differences [95% CI] were -5.7 [-29.6; +18.2] in Arm B, and +19.6 [-1.6; +40.8] in Arm C. A GRT was performed in 6/14 patients (one not amplifiable; four without mutations; one showed E138A).
Compared to maintaining a PI/r-based triple ARV regimen, LPV/r QD monotherapy tended to have higher rate of virological failure and of discontinuation due to adverse event. In contrast, the response rate at week 96 during DRV/r QD mono-therapy was non-inferior to that of triple PI/r-based ARV therapy. A re-induction with 2NRTI was adequate to obtain an undetectable viremia in most of patients with virological failure.
对于血浆中HIV得到稳定抑制的患者,蛋白酶抑制剂/利托那韦(PI/r)单药治疗被认为是一种可行的维持治疗策略。本试验的目的是比较两种不同的PI/r每日一次单药治疗策略(洛匹那韦/利托那韦或地瑞那韦/利托那韦)与维持基于三联PI/r的抗逆转录病毒治疗方案的病毒学结果。
一项III期、开放标签、非劣效性(非劣效界值为-12%)、随机试验,纳入血浆HIV-RNA<50拷贝/mL至少48周、接受基于PI/r的抗逆转录病毒治疗(cART)、CD4最低点>100个细胞/mm³且既往无PI病毒学失败的成年HIV患者。符合条件的患者被随机分配至继续接受PI/r+2种核苷类逆转录酶抑制剂(NRTIs)(A组),或转换为洛匹那韦/利托那韦800/200mg每日一次单药治疗(B组),或转换为地瑞那韦/利托那韦800/100mg每日一次单药治疗(C组)。主要终点是在意向性治疗(ITT)分析(缺失/重新诱导=失败)下48周时血浆HIV-1RNA<50拷贝/mL的患者比例。还采用了FDA快照分析和ITT纳入分析(ITT-SI)。在ITT-SI中,96周时HIV-RNA<50拷贝/mL的患者即使确认HIV-RNA升高且随后通过NRTI成功强化治疗,也被计为成功。
由于招募缓慢,仅纳入了103例患者。三组在性别、年龄、HIV传播途径、CD4最低点及筛查时均未观察到差异。随机分组时,61例患者接受替诺福韦酯/恩曲他滨(60%),19例接受齐多夫定/拉米夫定(18%),8例接受阿巴卡韦/拉米夫定(8%),75例接受洛匹那韦/利托那韦(73%),13例接受阿扎那韦/利托那韦(13%),4例接受地瑞那韦/利托那韦(4%)。图1报告了以A组为对照,根据FDA TLOVR分组的病毒学成功比例差异。快照分析得到了类似结果。在14例病毒学失败的患者中,8例患者重新开始三联治疗加2种NRTIs,其中7/8患者随时间推移病毒载量重新降至<50拷贝/mL。根据ITT-SI分析,B组96周差异[95%置信区间]为-5.7[-29.6;+18.2],C组为+19.6[-1.6;+40.8]。对14例患者中的6例进行了基因型耐药检测(GRT)(1例无法扩增;4例无突变;1例显示E138A)。
与维持基于PI/r的三联抗逆转录病毒治疗方案相比,洛匹那韦/利托那韦每日一次单药治疗的病毒学失败率和因不良事件停药率往往更高。相比之下,地瑞那韦/利托那韦每日一次单药治疗第96周时的缓解率不劣于基于三联PI/r的抗逆转录病毒治疗。对大多数病毒学失败的患者,加用2种NRTIs重新诱导治疗足以实现病毒血症不可检测。