Bron Morgan, Wilson Craig, Fleck Penny
Takeda Pharmaceuticals International, One Takeda Parkway, Deerfield, IL, 60015, USA,
Diabetes Ther. 2014 Dec;5(2):521-34. doi: 10.1007/s13300-014-0088-5. Epub 2014 Nov 26.
Adverse events and complications limit the long-term use of current antidiabetic treatment options for patients with type 2 diabetes mellitus (T2DM), particularly for older adults who are often receiving therapy for other comorbid conditions. The aim of this study was to evaluate the benefits of the dipeptidyl peptidase-4 inhibitor, alogliptin, versus glipizide, a sulfonylurea, in achieving glycemic control without the risk of hypoglycemia, weight gain, or both in older patients with T2DM.
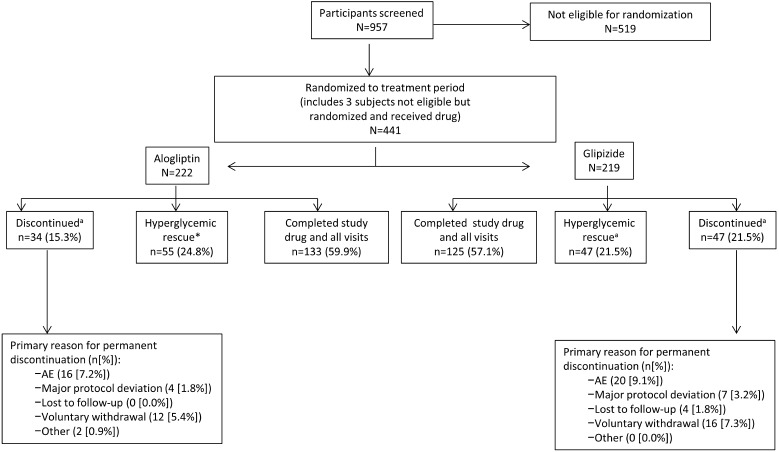
This was an exploratory, post hoc analysis of a global, multicenter, randomized, double-blind, active-controlled study comparing alogliptin and glipizide. Patients (n = 441) aged 65-90 years with glycosylated hemoglobin (HbA1c) 6.5-9.0% who failed on diet and exercise alone or who had inadequately controlled T2DM despite oral antidiabetic monotherapy were recruited from 110 sites across 15 countries. Alogliptin 25 mg (n = 222) or glipizide 5 mg up-titrated to 10 mg (n = 219) was administered once daily for 52 weeks. Composite endpoints of HbA1c ≤7.0% coupled with the absence of hypoglycemia and weight gain, or an HbA1c reduction of ≥0.5% in the absence of hypoglycemia and weight gain, were then measured.
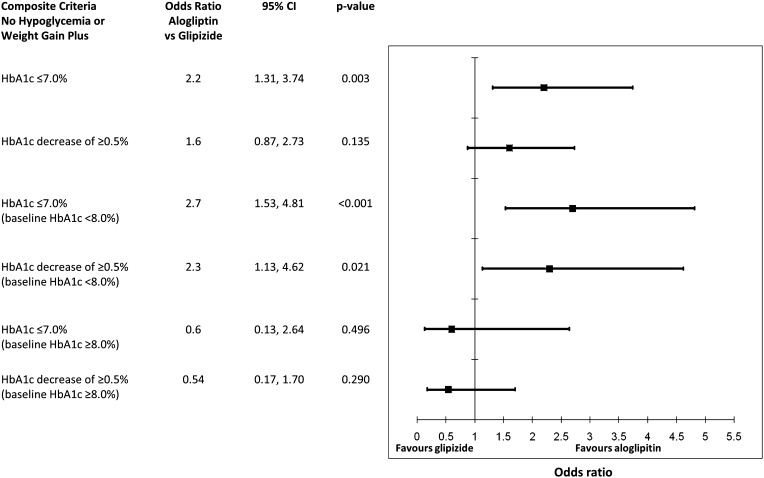
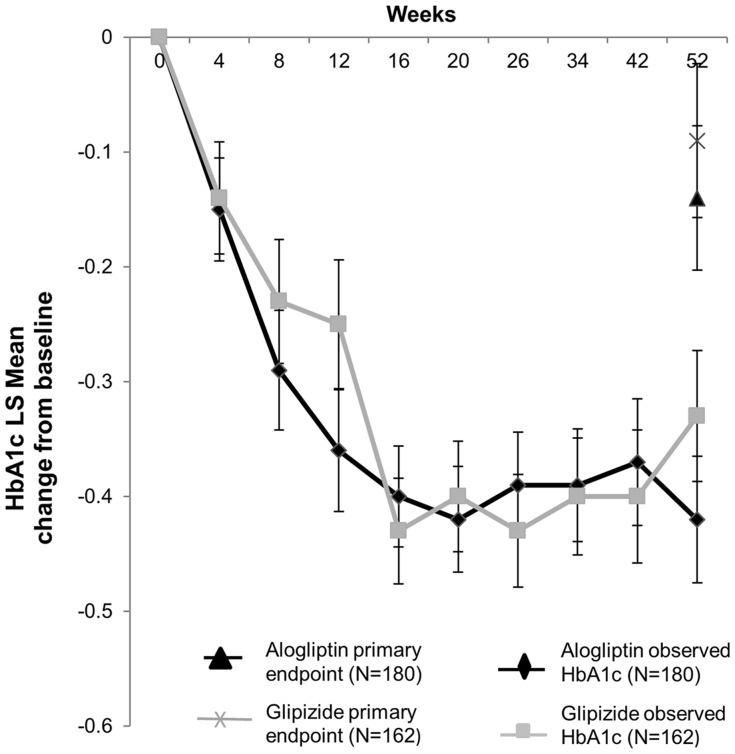
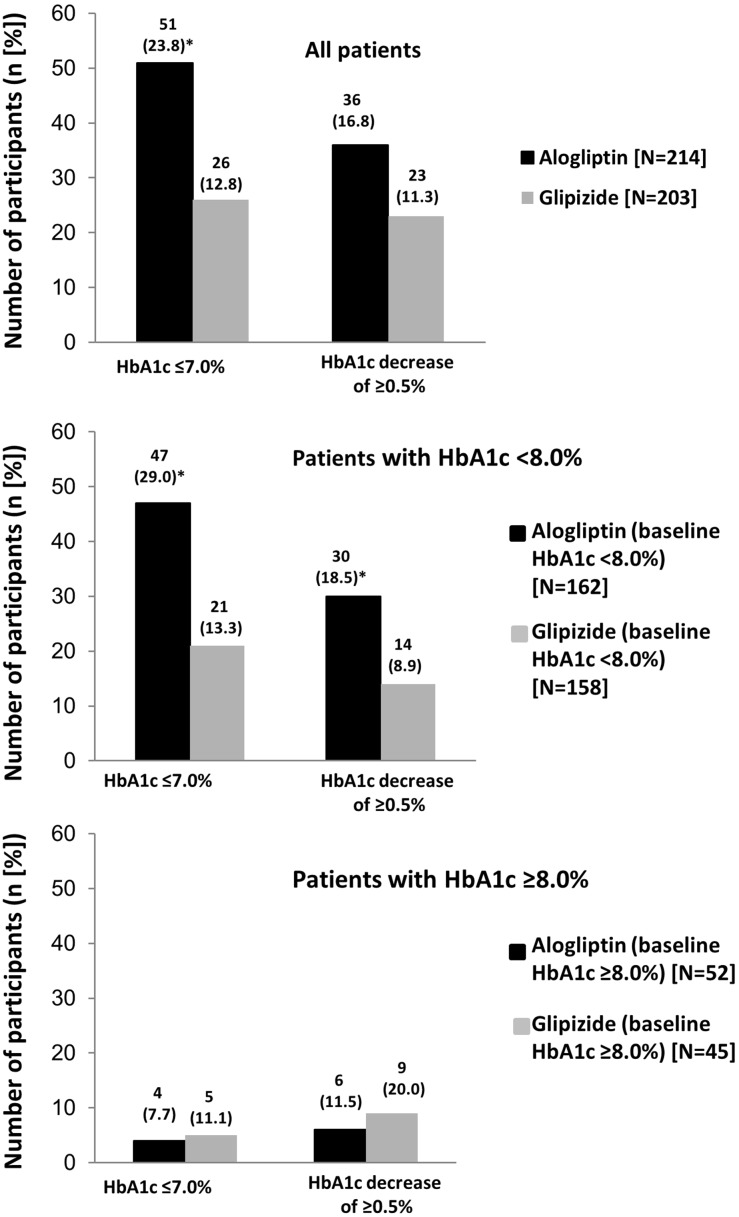
In the primary analysis, least squares mean HbA1c changes from baseline to Week 52 were similar in both the alogliptin and glipizide groups. The proportion of patients achieving HbA1c ≤7.0% without hypoglycemia or weight gain was significantly higher for alogliptin versus glipizide (24% vs 13%, p < 0.03). Patients with a baseline HbA1c of <8.0% receiving alogliptin were also more likely to achieve HbA1c ≤7.0% without hypoglycemia or weight gain than those receiving glipizide (29% vs 13%, p < 0.03).
Alogliptin demonstrated similar efficacy to glipizide in lowering HbA1c in older patients with T2DM, but with significantly more patients achieving an HbA1c ≤7.0% without hypoglycemia or an increase in body weight. These results particularly apply to patients with baseline HbA1c below 8.0%.
The study was sponsored by Takeda Global Research & Development Center, Inc., Deerfield, IL, and Takeda Global Research and Development Centre Ltd., London, United Kingdom.
不良事件和并发症限制了目前2型糖尿病(T2DM)患者抗糖尿病治疗方案的长期使用,尤其是对于那些常因其他合并症而接受治疗的老年人。本研究的目的是评估二肽基肽酶-4抑制剂阿格列汀与磺脲类药物格列吡嗪相比,在老年T2DM患者中实现血糖控制且无低血糖风险或体重增加的益处。
这是一项探索性的事后分析,基于一项全球多中心、随机、双盲、活性对照研究,比较阿格列汀和格列吡嗪。从15个国家的110个地点招募了年龄在65至90岁、糖化血红蛋白(HbA1c)为6.5 - 9.0%、仅通过饮食和运动治疗失败或尽管接受口服抗糖尿病单药治疗但T2DM控制不佳的患者(n = 441)。每日一次给予阿格列汀25 mg(n = 222)或格列吡嗪5 mg并滴定至10 mg(n = 219),持续52周。然后测量HbA1c≤7.0%且无低血糖和体重增加,或在无低血糖和体重增加的情况下HbA1c降低≥0.5%的复合终点。
在初步分析中,阿格列汀组和格列吡嗪组从基线到第52周的HbA1c最小二乘均值变化相似。阿格列汀组中在无低血糖或体重增加的情况下实现HbA1c≤7.0%的患者比例显著高于格列吡嗪组(24%对13%,p < 0.03)。基线HbA1c < 8.0%且接受阿格列汀治疗的患者比接受格列吡嗪治疗的患者更有可能在无低血糖或体重增加的情况下实现HbA1c≤7.0%(29%对13%,p < 0.03)。
在降低老年T2DM患者的HbA1c方面,阿格列汀显示出与格列吡嗪相似的疗效,但在无低血糖或体重增加的情况下实现HbA1c≤7.0%的患者显著更多。这些结果尤其适用于基线HbA1c低于8.0%的患者。
该研究由位于伊利诺伊州迪尔菲尔德的武田全球研发中心公司以及位于英国伦敦的武田全球研发中心有限公司赞助。