Institute for Maternal and Child Health, IRCCS "Burlo Garofolo", Trieste, Italy ; Department of Medical Sciences, University of Trieste, Trieste, Italy.
Department of Medical Sciences, University of Trieste, Trieste, Italy.
Ther Clin Risk Manag. 2014 Nov 17;10:963-8. doi: 10.2147/TCRM.S65634. eCollection 2014.
To report a case of Essure microinsert abdominal migration and literature review.
A 41-year-old woman was counseled to undergo Essure sterilization. The procedure was hampered by the presence of endometrial cavity adhesions, obscuring left tubal ostium. By using microscissors the adhesions were progressively lysed. Since the procedure had become very painful, the patient required general anesthesia. Once adhesion lysis was completed, the tubal ostium was well visible. Both devices were then easily introduced into the fallopian tubes. At the end of the procedure, five coils were visible on the right side and five coils on the left side, as recommended.
The 3-month hysterosalpingogram follow-up suspected abdominal migration of the left device. Laparoscopy confirmed the device displacement in the left lower abdominal quadrant. Both fallopian tubes and the uterus appeared normal. No signs of perforation were detected. The device was embedded into the omentum, but it was easily removed. Bilateral tubal sterilization was performed by bipolar coagulation.
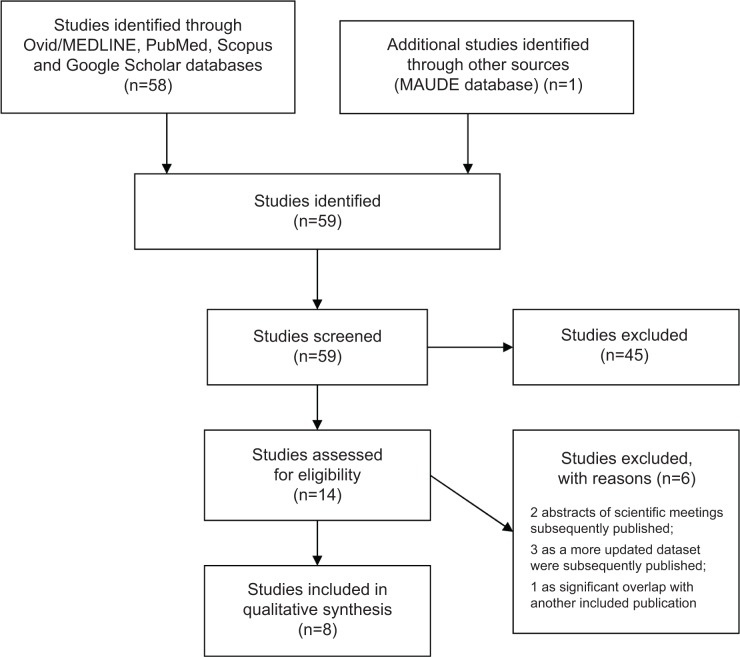
There are only 13 cases, including the present, of Essure abdominal migration in the literature. In most cases, abdominal displacement of the microinsert is asymptomatic and does not induce tissue damage. However, in some cases, it may cause a severe adverse event, requiring major surgery. Therefore, removal of the migrated device should be performed as soon as possible. Moreover, during presterilization counseling, the patient should also be correctly informed about the risk of this rare but relevant complication, as well as about the surgical interventions that could be required to solve it.
报告一例 Essure 微植入物腹部迁移病例并进行文献复习。
一名 41 岁女性接受 Essure 绝育咨询。由于存在子宫内膜腔粘连,左侧输卵管口被遮挡,手术过程受阻。通过使用显微剪刀逐渐松解粘连。由于手术过程非常疼痛,患者需要全身麻醉。一旦粘连松解完成,输卵管口就可以清晰可见。然后,很容易将两个装置引入输卵管。手术结束时,右侧可见 5 个线圈,左侧可见 5 个线圈,符合推荐标准。
术后 3 个月的子宫输卵管造影随访怀疑左侧装置发生腹部迁移。腹腔镜检查证实了设备在左下腹象限的位置发生了移位。双侧输卵管和子宫均正常,未发现穿孔迹象。该设备嵌入到了网膜中,但很容易被取出。通过双极电凝对双侧输卵管进行了绝育。
文献中仅有 13 例 Essure 腹部迁移病例,包括本病例。在大多数情况下,微植入物的腹部移位是无症状的,不会引起组织损伤。然而,在某些情况下,它可能会导致严重的不良事件,需要进行重大手术。因此,应尽快取出迁移的装置。此外,在绝育咨询中,还应正确告知患者这种罕见但相关的并发症风险,以及可能需要进行的手术干预来解决该问题。