Pilgrim Thomas, Rothenbühler Martina, Kalesan Bindu, Pulver Cédric, Stefanini Giulio G, Zanchin Thomas, Räber Lorenz, Stortecky Stefan, Jung Simon, Mattle Heinrich, Moschovitis Aris, Wenaweser Peter, Meier Bernhard, Gsponer Thomas, Windecker Stephan, Jüni Peter
Department of Cardiology, Swiss Cardiovascular Center, Bern University Hospital, Bern, Switzerland.
Institute of Social and Preventive Medicine and Clinical Trials Unit, University of Bern, Bern, Switzerland.
PLoS One. 2014 Dec 9;9(12):e114846. doi: 10.1371/journal.pone.0114846. eCollection 2014.
Anemia and renal impairment are important co-morbidities among patients with coronary artery disease undergoing Percutaneous Coronary Intervention (PCI). Disease progression to eventual death can be understood as the combined effect of baseline characteristics and intermediate outcomes.
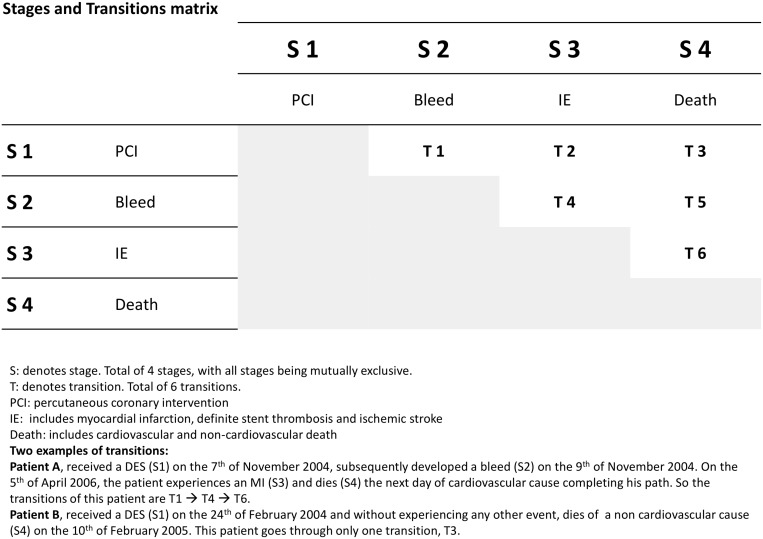
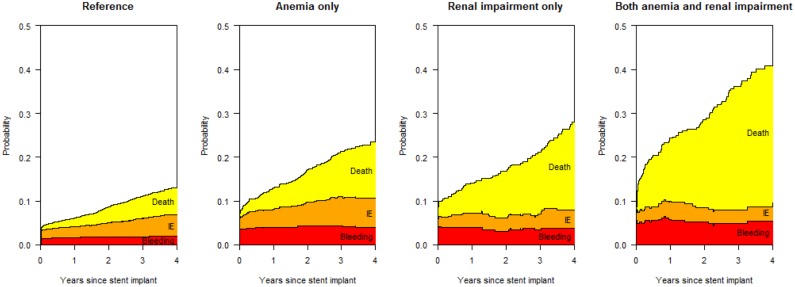
Using data from a prospective cohort study, we investigated clinical pathways reflecting the transitions from PCI through intermediate ischemic or hemorrhagic events to all-cause mortality in a multi-state analysis as a function of anemia (hemoglobin concentration <120 g/l and <130 g/l, for women and men, respectively) and renal impairment (creatinine clearance <60 ml/min) at baseline.
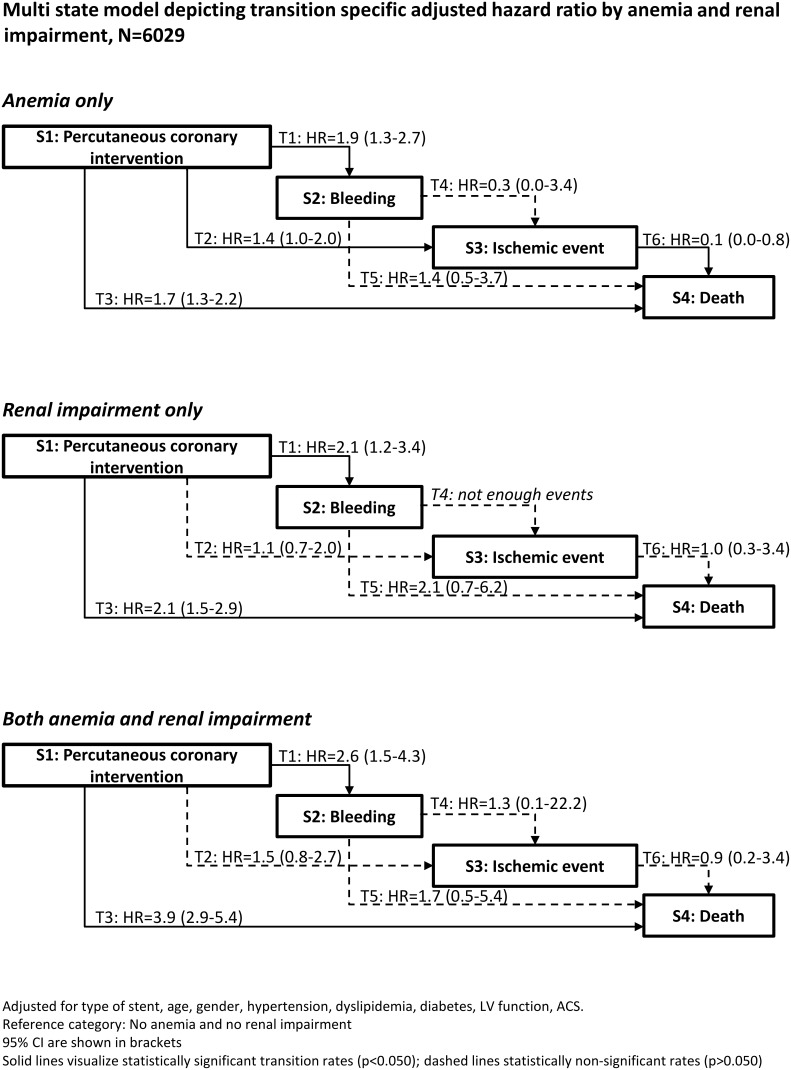
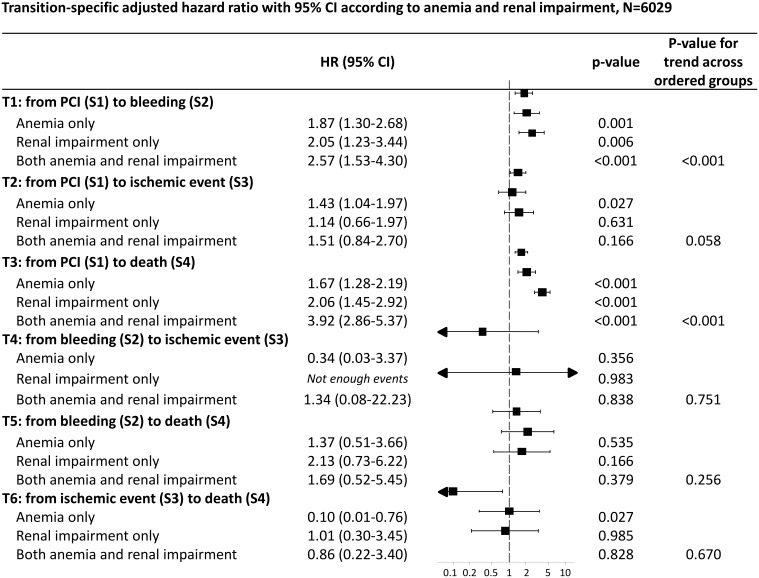
Among 6029 patients undergoing PCI, anemia and renal impairment were observed isolated or in combination in 990 (16.4%), 384 (6.4%), and 309 (5.1%) patients, respectively. The most frequent transition was from PCI to death (6.7%, 95% CI 6.1-7.3), followed by ischemic events (4.8%, 95 CI 4.3-5.4) and bleeding (3.4%, 95% CI 3.0-3.9). Among patients with both anemia and renal impairment, the risk of death was increased 4-fold as compared to the reference group (HR 3.9, 95% CI 2.9-5.4) and roughly doubled as compared to patients with either anemia (HR 1.7, 95% CI 1.3-2.2) or renal impairment (HR 2.1, 95% CI 1.5-2.9) alone. Hazard ratios indicated an increased risk of bleeding in all three groups compared to patients with neither anemia nor renal impairment.
Applying a multi-state model we found evidence for a gradient of risk for the composite of bleeding, ischemic events, or death as a function of hemoglobin value and estimated glomerular filtration rate at baseline.
贫血和肾功能损害是接受经皮冠状动脉介入治疗(PCI)的冠心病患者中重要的合并症。疾病进展至最终死亡可理解为基线特征和中间结局的综合影响。
利用一项前瞻性队列研究的数据,我们在多状态分析中研究了反映从PCI经中间缺血或出血事件至全因死亡的临床路径,该分析将贫血(女性血红蛋白浓度<120 g/l,男性<130 g/l)和基线时的肾功能损害(肌酐清除率<60 ml/min)作为函数。
在6029例接受PCI的患者中,分别有990例(16.4%)、384例(6.4%)和309例(5.1%)患者单独或合并出现贫血和肾功能损害。最常见的转变是从PCI至死亡(6.7%,95%CI 6.1-7.3),其次是缺血事件(4.8%,95%CI 4.3-5.4)和出血(3.4%,95%CI 3.0-3.9)。在同时患有贫血和肾功能损害的患者中,与参照组相比死亡风险增加了4倍(HR 3.9,95%CI 2.9-5.4),与单独患有贫血(HR 1.7,95%CI 1.3-2.2)或肾功能损害(HR 2.1,95%CI 1.5-2.9)的患者相比风险大致增加了一倍。风险比表明,与既无贫血也无肾功能损害的患者相比,所有三组出血风险均增加。
应用多状态模型,我们发现有证据表明,根据基线血红蛋白值和估计的肾小球滤过率来看,出血、缺血事件或死亡综合风险呈梯度变化。