Yahya Noorazrul, Ebert Martin A, Bulsara Max, Haworth Annette, Kearvell Rachel, Foo Kerwyn, Kennedy Angel, Richardson Sharon, Krawiec Michele, Joseph David J, Denham Jim W
School of Physics, University of Western Australia, Crawley, Western Australia, Australia.
School of Health Sciences, National University of Malaysia, Bangi, Malaysia.
Radiat Oncol. 2014 Dec 13;9:282. doi: 10.1186/s13014-014-0282-7.
To assess the impact of incremental modifications of treatment planning and delivery technique, as well as patient anatomical factors, on late gastrointestinal toxicity using data from the TROG 03.04 RADAR prostate radiotherapy trial.
The RADAR trial accrued 813 external beam radiotherapy participants during 2003-2008 from 23 centres. Following review and archive to a query-able database, digital treatment plans and data describing treatment technique for 754 patients were available for analysis. Treatment demographics, together with anatomical features, were assessed using uni- and multivariate regression models against late gastrointestinal toxicity at 18-, 36- and 54-month follow-up. Regression analyses were reviewed in the context of dose-volume data for the rectum and anal canal.
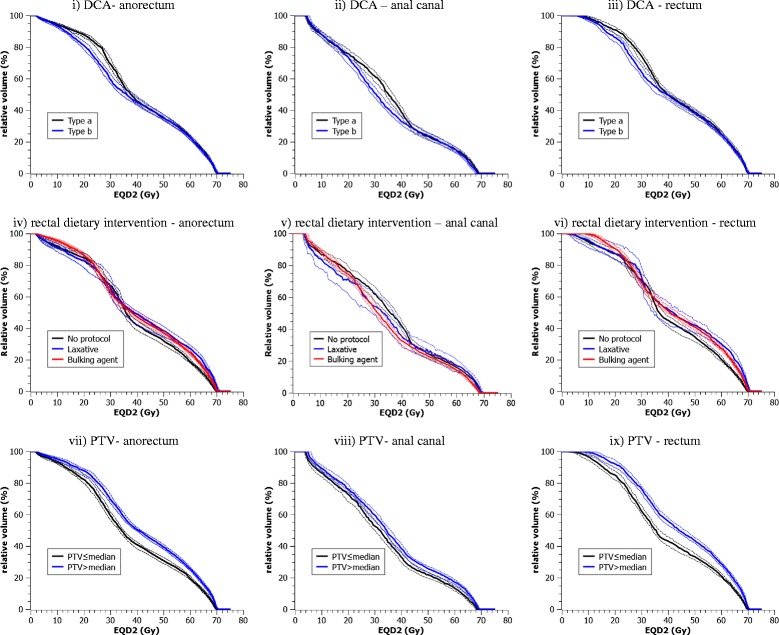
A multivariate analysis at 36-month follow-up shows that patients planned using a more rigorous dose calculation algorithm (DCA) was associated with a lower risk of stool frequency (OR: 0.435, CI: 0.242-0.783, corrected p = 0.04). Patients using laxative as a method of bowel preparation had higher risk of having increased stool frequency compared to patients with no dietary intervention (OR: 3.639, CI: 1.502-8.818, corrected p = 0.04). Despite higher risks of toxicities, the anorectum, anal canal and rectum dose-volume histograms (DVH) indicate patients using laxative had unremarkably different planned dose distributions. Patients planned with a more rigorous DCA had lower median DVH values between EQD23 = 15 Gy and EQD23 = 35 Gy. Planning target volume (PTV), conformity index, rectal width and prescription dose were not significant when adjusted for false discovery rate. Number of beams, beam energy, treatment beam definition, positioning orientation, rectum-PTV separation, rectal length and mean cross sectional area did not affect the risk of toxicities.
The RADAR study dataset has allowed an assessment of technical modifications on gastrointestinal toxicity. A number of interesting associations were subsequently found and some factors, previously hypothesised to influence toxicity, did not demonstrate any significant impact. We recommend trial registries be encouraged to record technical modifications introduced during the trial in order for more powerful evidence to be gathered regarding the impact of the interventions.
利用TROG 03.04 RADAR前列腺放射治疗试验的数据,评估治疗计划和实施技术的逐步改进以及患者解剖因素对晚期胃肠道毒性的影响。
RADAR试验在2003年至2008年期间从23个中心招募了813名接受外照射放疗的参与者。在对数据进行审查并存档到可查询数据库后,获得了754名患者的数字治疗计划和描述治疗技术的数据,用于分析。使用单变量和多变量回归模型,在18个月、36个月和54个月的随访中,评估治疗人口统计学数据以及解剖特征与晚期胃肠道毒性的关系。在直肠和肛管剂量体积数据的背景下对回归分析进行了审查。
在36个月随访时的多变量分析表明,使用更严格剂量计算算法(DCA)进行计划的患者,大便频率风险较低(比值比:0.435,可信区间:0.242 - 0.783,校正p = 0.04)。与未进行饮食干预的患者相比,使用泻药作为肠道准备方法的患者大便频率增加的风险更高(比值比:3.639,可信区间:1.502 - 8.818,校正p = 0.04)。尽管毒性风险较高,但肛门直肠、肛管和直肠的剂量体积直方图(DVH)表明,使用泻药的患者计划剂量分布并无明显差异。使用更严格DCA进行计划的患者,在等效剂量2(EQD2)为15 Gy至35 Gy之间的DVH中位数较低。在调整错误发现率后,计划靶体积(PTV)、适形指数、直肠宽度和处方剂量并不显著。射野数量、射野能量、治疗射野定义、定位方向、直肠与PTV的间距、直肠长度和平均横截面积均不影响毒性风险。
RADAR研究数据集使得对胃肠道毒性的技术改进评估成为可能。随后发现了一些有趣的关联,并且一些先前假设会影响毒性的因素并未显示出任何显著影响。我们建议鼓励试验注册机构记录试验期间引入的技术改进,以便收集关于干预措施影响的更有力证据。