Chou Angela, Fraser Sheila, Toon Christopher W, Clarkson Adele, Sioson Loretta, Farzin Mahtab, Cussigh Carmen, Aniss Ahmad, O'Neill Christine, Watson Nicole, Clifton-Bligh Roderick J, Learoyd Diana L, Robinson Bruce G, Selinger Christina I, Delbridge Leigh W, Sidhu Stanley B, O'Toole Sandra A, Sywak Mark, Gill Anthony J
*Cancer Diagnosis and Pathology Research Group §§Sydney Vital Translational Research Centre, Kolling Institute of Medical Research §University of Sydney Endocrine Surgical Unit **Hormones and Cancer Group, Cancer Genetics Laboratory, Kolling Institute of Medical Research Departments of ¶Anatomical Pathology #Endocrinology, Royal North Shore Hospital, St Leonards †Department of Anatomical Pathology SYDPATH, St Vincent's Hospital ‡Kinghorn Cancer Centre and Cancer Research Program, Garvan Institute of Medical Research, Darlinghurst ∥Histopath Pathology, North Ryde ††Department of Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Camperdown ‡‡University of Sydney, Sydney, NSW, Australia.
Am J Surg Pathol. 2015 May;39(5):652-9. doi: 10.1097/PAS.0000000000000368.
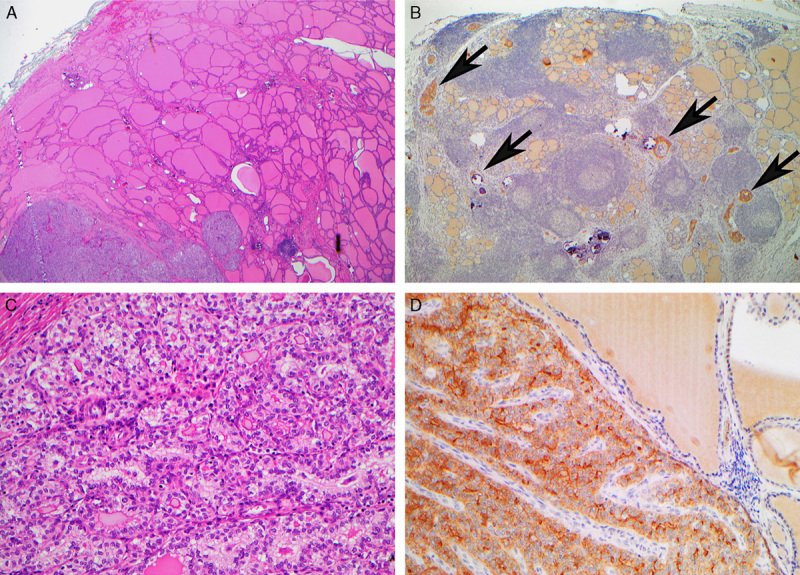
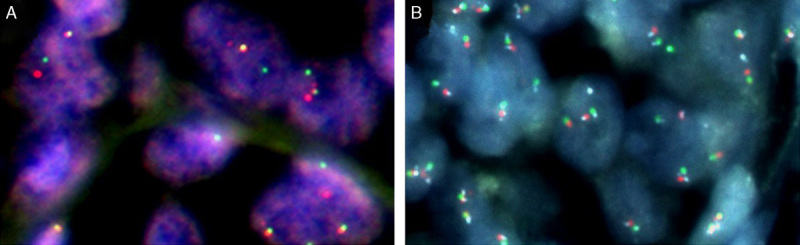
Pathogenic ALK translocations have been reported in papillary thyroid carcinoma (PTC). We developed and validated a screening algorithm based on immunohistochemistry (IHC), followed by fluorescence in situ hybridization (FISH) in IHC-positive cases to identify ALK-rearranged PTC. IHC and FISH were performed in a cohort of 259 thyroid carcinomas enriched for aggressive variants. IHC was positive in 8 cases, 6 confirmed translocated by FISH (specificity 75%). All 251 IHC-negative cases were FISH negative (sensitivity 100%). Having validated this approach, we performed screening IHC, followed by FISH in IHC-positive cases in an expanded cohort. ALK translocations were identified in 11 of 498 (2.2%) of all consecutive unselected PTCs and 3 of 23 (13%) patients with diffuse sclerosing variant PTCs. No ALK translocations were identified in 36 PTCs with distant metastases, 28 poorly differentiated (insular) carcinomas, and 20 anaplastic carcinomas. All 14 patients with ALK translocations were female (P=0.0425), and translocations occurred at a younger age (mean 38 vs. 48 y, P=0.0289 in unselected patients). ALK translocation was an early clonal event present in all neoplastic cells and mutually exclusive with BRAF mutation. ALK translocation was not associated with aggressive clinicopathologic features (size, stage, metastasis, vascular invasion, extrathyroidal extension, multifocality, risk for recurrence, radioiodine resistance). We conclude that 2.2% of PTCs are ALK-translocated and can be identified by screening IHC followed by FISH. ALK translocations may be more common in young females and diffuse sclerosing variant PTC but do not connote more aggressive disease.
在乳头状甲状腺癌(PTC)中已报道有致病性ALK易位。我们开发并验证了一种基于免疫组织化学(IHC)的筛查算法,在IHC阳性病例中随后进行荧光原位杂交(FISH)以鉴定ALK重排的PTC。对一组259例富含侵袭性变体的甲状腺癌进行了IHC和FISH检测。8例IHC呈阳性,其中6例经FISH证实为易位(特异性75%)。所有251例IHC阴性病例FISH均为阴性(敏感性100%)。在验证了该方法后,我们在一个扩大的队列中进行了筛查IHC,然后对IHC阳性病例进行FISH检测。在所有连续入选的498例PTC中有11例(2.2%)以及23例弥漫性硬化变体PTC患者中有3例(13%)检测到ALK易位。在36例有远处转移的PTC、28例低分化(岛状)癌和20例未分化癌中未检测到ALK易位。所有14例ALK易位患者均为女性(P = 0.0425),且易位发生在较年轻的年龄(未入选患者中平均年龄38岁对48岁,P = 0.0289)。ALK易位是所有肿瘤细胞中存在的早期克隆事件,且与BRAF突变相互排斥。ALK易位与侵袭性临床病理特征(大小、分期、转移、血管侵犯、甲状腺外扩展、多灶性、复发风险、放射性碘抵抗)无关。我们得出结论,2.2%的PTC存在ALK易位,可通过先筛查IHC然后进行FISH来识别。ALK易位在年轻女性和弥漫性硬化变体PTC中可能更常见,但并不意味着疾病更具侵袭性。