Vavallo Antonio, Simone Simona, Lucarelli Giuseppe, Rutigliano Monica, Galleggiante Vanessa, Grandaliano Giuseppe, Gesualdo Loreto, Campagna Marcello, Cariello Marica, Ranieri Elena, Pertosa Giovanni, Lastilla Gaetano, Selvaggi Francesco Paolo, Ditonno Pasquale, Battaglia Michele
From the Department of Emergency and Organ Transplantation, Urology, Andrology and Kidney Transplantation Unit, University of Bari, Bari (AV, GL, MR, VG, MC, PS, PD, MB); Department of Medical and Surgical Sciences, Nephrology, Dialysis and Transplantation Unit, University of Foggia, Foggia (GG, ER); Department of Emergency and Organ Transplantation - Nephrology, Dialysis and Transplantation Unit (SS, MC, GP); and Department of Pathology, University of Bari, Bari, Italy (GL).
Medicine (Baltimore). 2014 Dec;93(27):e183. doi: 10.1097/MD.0000000000000183.
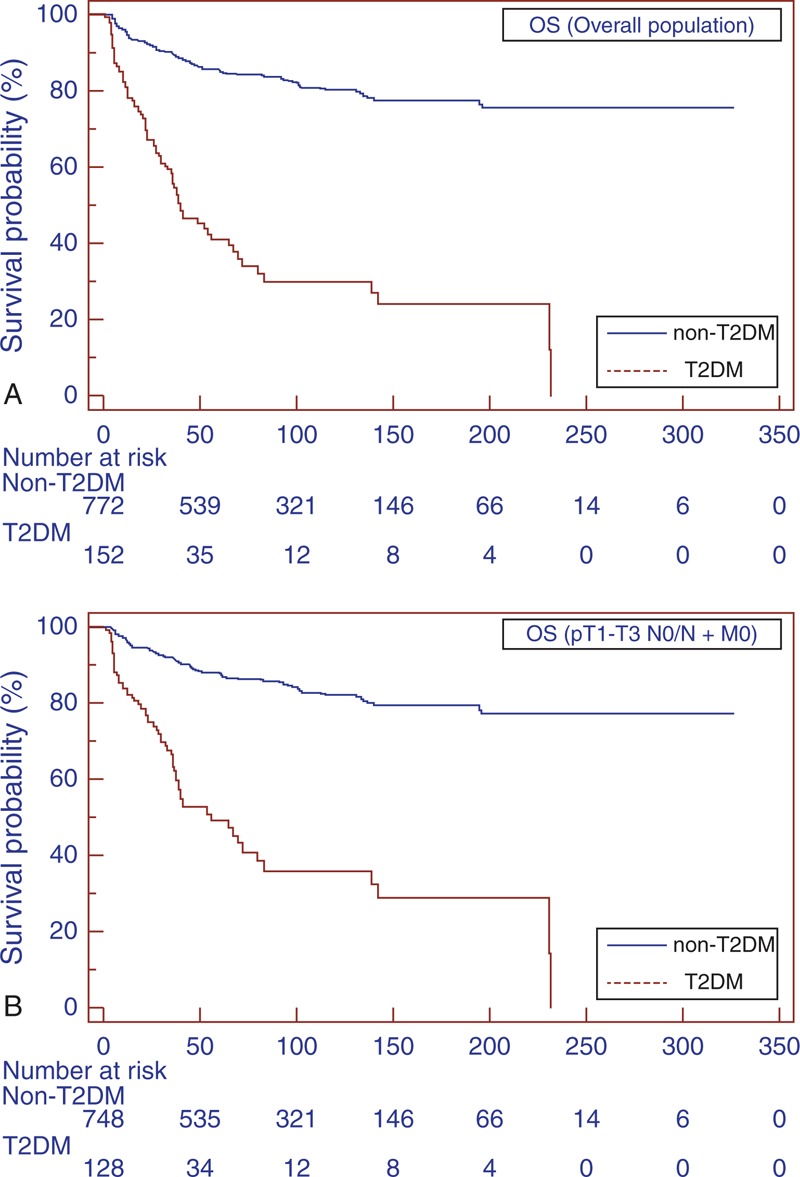
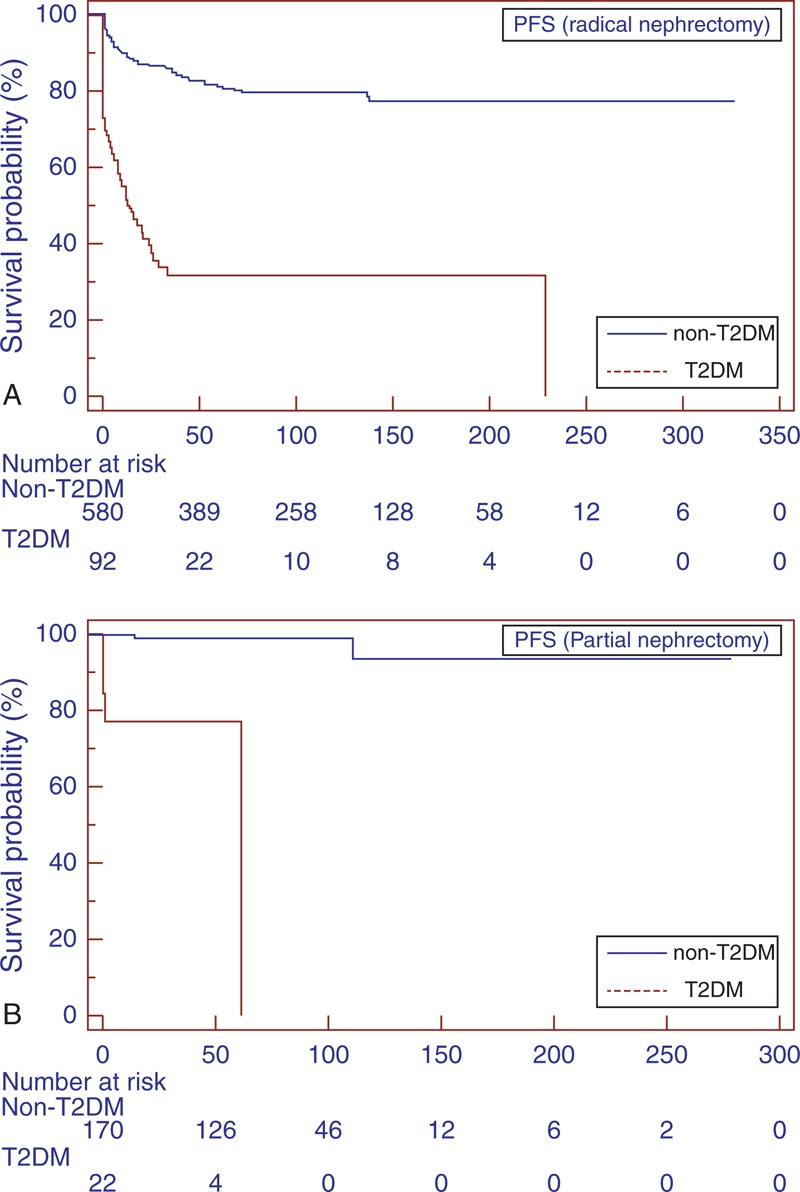
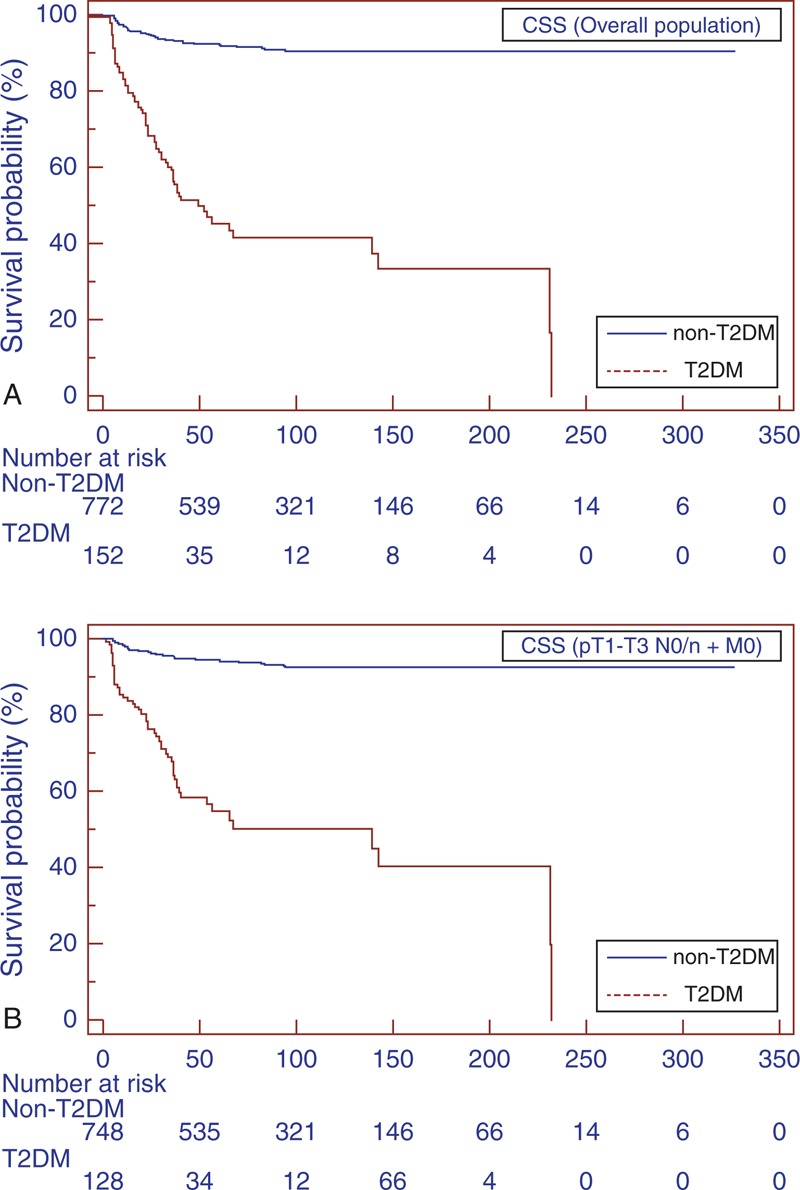
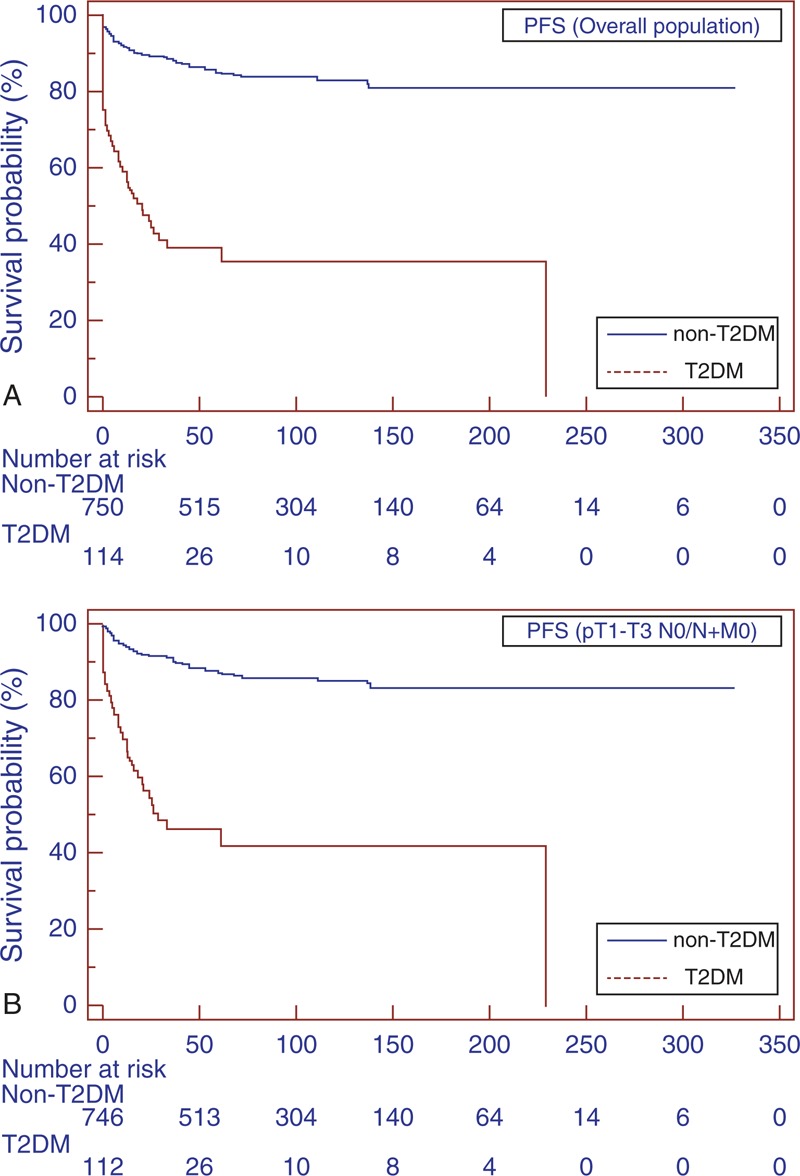
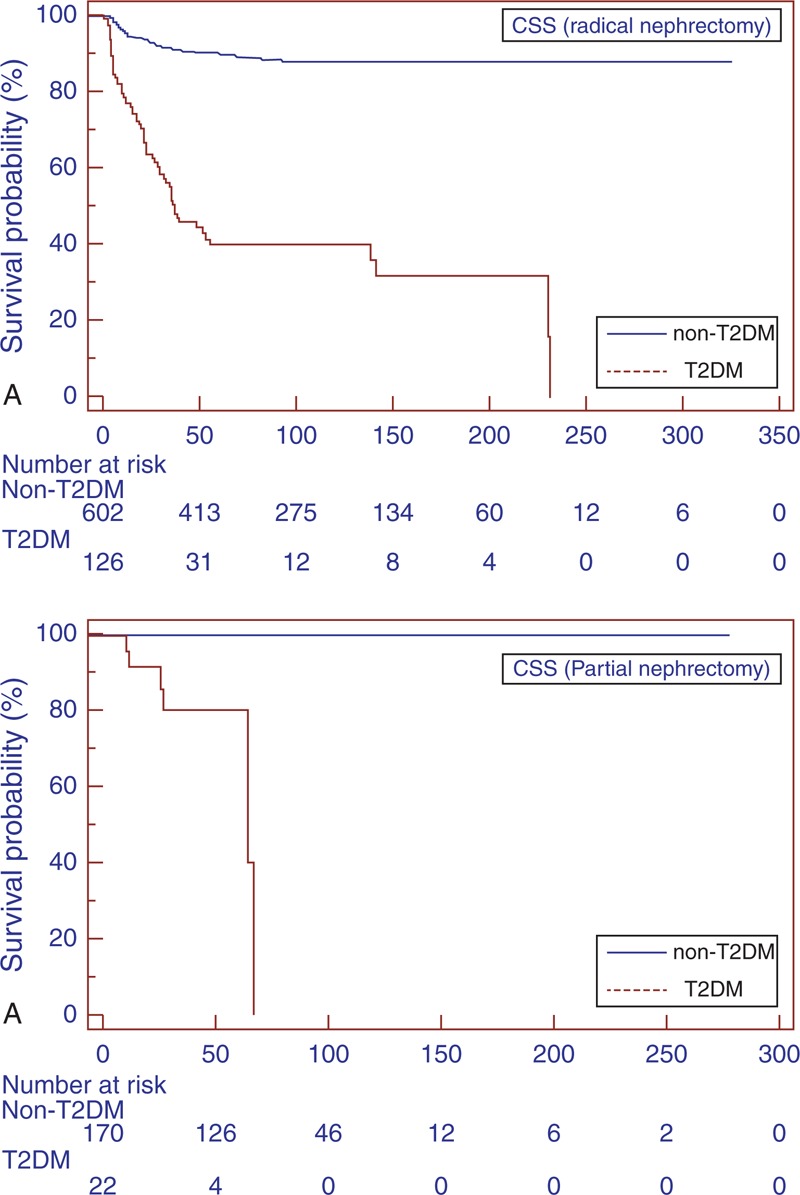
Malignancies are one of the main causes of mortality in diabetic patients; however, to date, very limited data have been reported on the specific influence of type 2 diabetes mellitus (T2DM) on the survival of patients with renal cell carcinoma (RCC). In the present long-term retrospective study, we investigated whether T2DM may influence the overall survival (OS), cancer-specific survival (CSS), and progression-free survival (PFS) in patients with surgically treated RCC. Medical records of 924 patients treated by radical or partial nephrectomy for sporadic, unilateral RCC were reviewed. Patients with type-1 DM and with T2 DM receiving insulin treatment were excluded. Survival estimates were calculated according to the Kaplan-Meier method and compared with the log-rank test. Univariate and multivariate analyses were performed using the Cox regression model.Of the 924 RCC patients, 152 (16.5%) had T2DM. Mean follow-up was 68.5 months. Mean OS was 41.3 and 96.3 months in T2DM and non-T2DM patients, respectively (P < 0.0001).The estimated CSS rates at 1, 3, and 5 years in T2DM versus non-T2DM patients were 63.4% versus 76.7%, 30.4% versus 56.6%, and 16.3% versus 48.6%, respectively (P = 0.001). Mean PFS was significantly lower (31.5 vs 96.3 months; P < 0.0001) in the T2DM group. At multivariate analysis, T2DM was an independent adverse prognostic factor for OS (hazard ratio [HR] = 3.44; 95% confidence interval [CI]:2.40-4.92), CSS (HR = 6.39; 95% CI: 3.78-10.79), and PFS (HR = 4.71; 95% CI: 3.11-7.15). In conclusion, our findings suggest that patients with RCC and pre-existing T2DM have a shorter OS, increased risk of recurrence, and higher risk for kidney cancer mortality than those without diabetes.
恶性肿瘤是糖尿病患者死亡的主要原因之一;然而,迄今为止,关于2型糖尿病(T2DM)对肾细胞癌(RCC)患者生存率的具体影响的报道非常有限。在本项长期回顾性研究中,我们调查了T2DM是否会影响接受手术治疗的RCC患者的总生存期(OS)、癌症特异性生存期(CSS)和无进展生存期(PFS)。我们回顾了924例因散发性、单侧RCC接受根治性或部分肾切除术治疗的患者的病历。排除1型糖尿病患者和接受胰岛素治疗的T2DM患者。根据Kaplan-Meier方法计算生存估计值,并与对数秩检验进行比较。使用Cox回归模型进行单因素和多因素分析。在924例RCC患者中,152例(16.5%)患有T2DM。平均随访时间为68.5个月。T2DM患者和非T2DM患者的平均OS分别为41.3个月和96.3个月(P<0.0001)。T2DM患者与非T2DM患者1年、3年和5年的CSS估计率分别为63.4%对76.7%、30.4%对56.6%和16.3%对48.6%(P=0.001)。T2DM组的平均PFS显著更低(31.5个月对96.3个月;P<0.0001)。在多因素分析中,T2DM是OS(风险比[HR]=3.44;95%置信区间[CI]:2.40-4.92)、CSS(HR=6.39;95%CI:3.78-10.79)和PFS(HR=4.71;95%CI:3.11-7.15)的独立不良预后因素。总之,我们的研究结果表明,与无糖尿病的患者相比,患有RCC且已患T2DM的患者OS更短,复发风险增加,肾癌死亡风险更高。