Chung Tzu-Chun, Yang Shih-Chieh, Chen Hung-Shu, Kao Yu-Hsien, Tu Yuan-Kun, Chen Wen-Jer
From the Department of Orthopaedic Surgery and Anesthesiology (T-CC, S-CY, H-SC, Y-HK, Y-KT), E-Da Hospital, I-Shou University, Kaohsiung; and Department of Orthopaedic Surgery (W-JC), Chang Gung Memorial Hospital, Taoyuan, Taiwan.
Medicine (Baltimore). 2014 Dec;93(27):e190. doi: 10.1097/MD.0000000000000190.
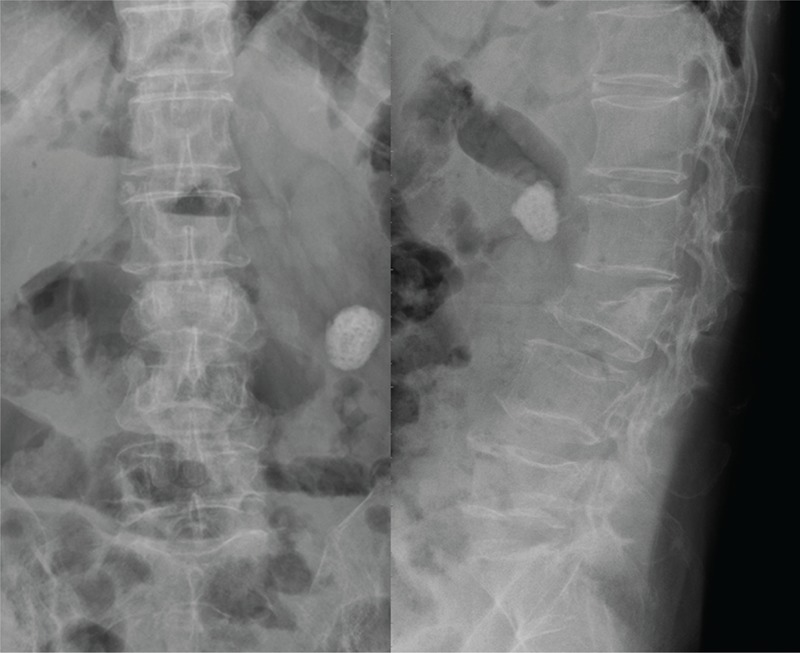
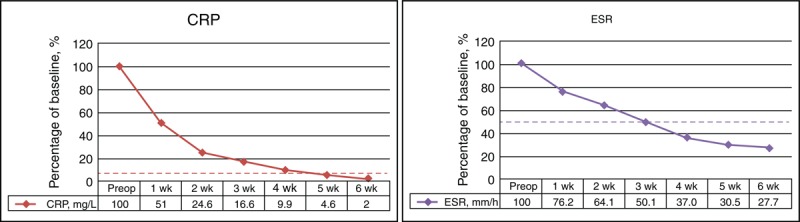
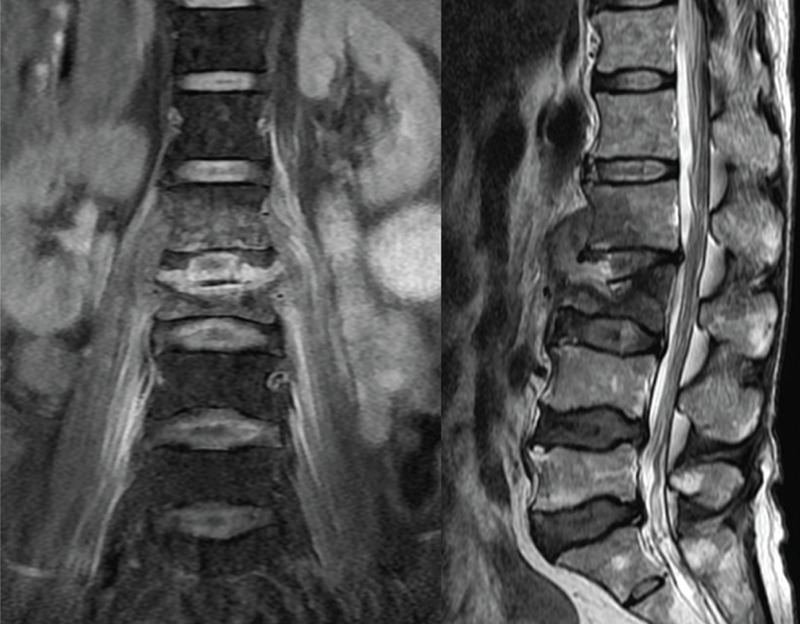
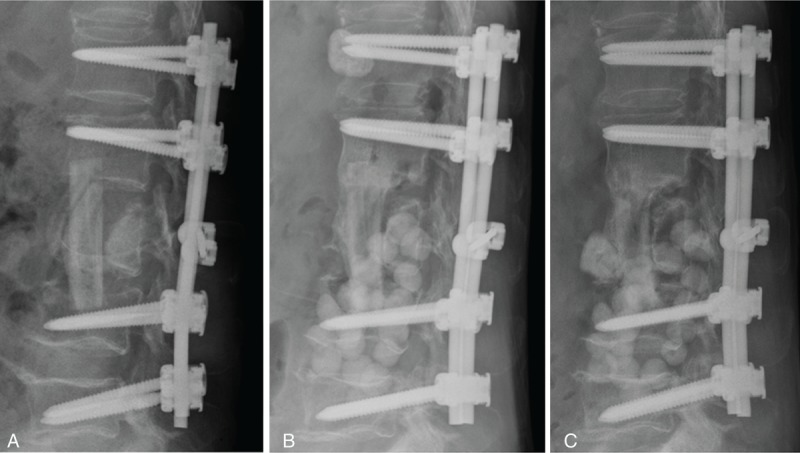
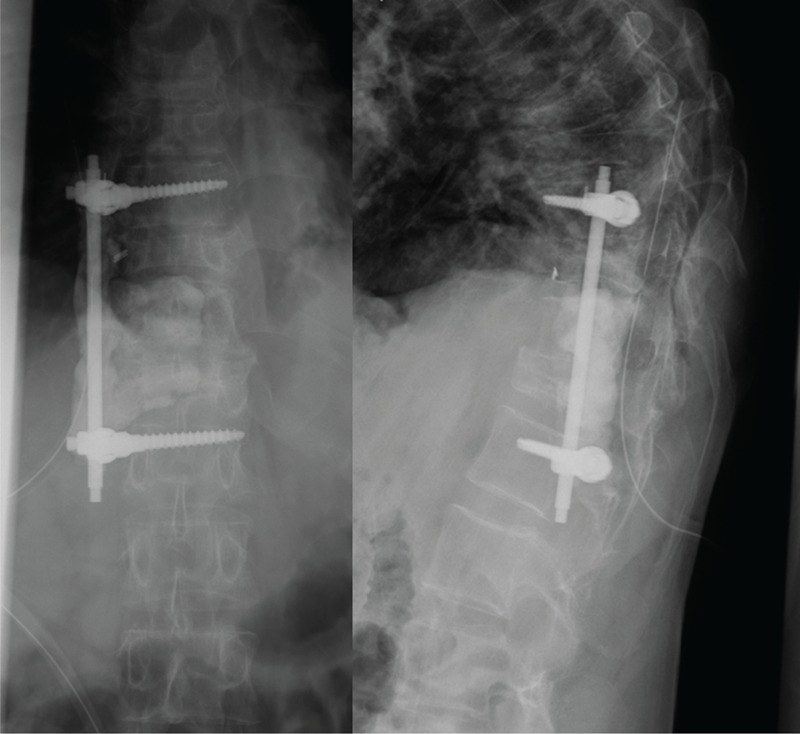
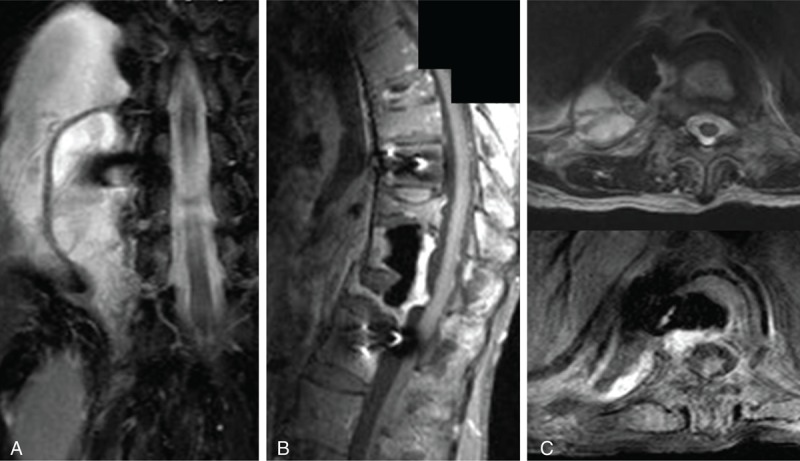
Complicated infectious spondylitis is an infrequent infection with severe spinal destruction, and is indicated for combined anterior and posterior surgeries. Staged debridement and subsequent reconstruction is advocated in the literature. The purpose of this study is to evaluate the feasibility and clinical outcome of patients who underwent single-stage combined anterior debridement and fibular allograft implantation followed by supplemental posterior fixation for complicated infectious spondylitis. We retrospectively reviewed the medical records of 20 patients who underwent single-stage combined anterior and posterior surgeries for complicated infectious spondylitis from January 2005 to December 2010. Complicated infectious spondylitis was defined as at least 1 vertebral osteomyelitis with pathological fracture or severe bony destruction and adjacent discitis, based on imaging studies. The severity of the neurological status was evaluated using the Frankel scale. The clinical outcomes were assessed by careful physical examination and regular serological tests to determine the visual analog scale (VAS) score and Macnab criteria. Correction of the sagittal Cobb angle on radiography was also compared before and after surgery. The Wilcoxon signed-rank test was used to analyze patient surgical prognosis and radiological findings. All patients with complicated infectious spondylitis were successfully treated by single-stage combined anterior and posterior surgeries. No patients experienced neurologic deterioration. The average VAS score was 7.8 before surgery and significantly decreased to 2.1 at discharge. Three patients had excellent outcomes and 17 had good outcomes, based on Macnab criteria. The average length of the allograft for reconstruction was 64.0 mm. Kyphotic deformity improved in all patients, with an average correction angle of 13.4°. There was no implant breakage or allograft dislodgement during at least 36 months of follow-up. Single-stage anterior debridement and fibular allograft implantation followed by posterior pedicle screw instrumentation provide immediate stability, satisfactory alignment, and successful infection control. Fibular allograft implantation seems to be a good alternative for anterior reconstruction; it can proceed to bony incorporation and avoids donor site morbidity.
复杂性感染性脊柱炎是一种罕见的感染性疾病,伴有严重的脊柱破坏,需行前后联合手术治疗。文献中提倡分期清创及后续重建手术。本研究旨在评估接受一期前路清创、腓骨异体骨移植并辅以后路固定治疗复杂性感染性脊柱炎患者的可行性及临床疗效。我们回顾性分析了2005年1月至2010年12月期间接受一期前后联合手术治疗复杂性感染性脊柱炎的20例患者的病历资料。根据影像学检查,复杂性感染性脊柱炎定义为至少1处椎体骨髓炎合并病理性骨折或严重骨质破坏及相邻椎间盘炎。采用Frankel分级评估神经功能状态的严重程度。通过仔细的体格检查和定期的血清学检查评估临床疗效,以确定视觉模拟评分(VAS)及Macnab标准。同时比较手术前后X线片上矢状面Cobb角的矫正情况。采用Wilcoxon符号秩和检验分析患者的手术预后及影像学表现。所有复杂性感染性脊柱炎患者均通过一期前后联合手术成功治疗。无患者出现神经功能恶化。术前平均VAS评分为7.8分,出院时显著降至2.1分。根据Macnab标准,3例患者疗效为优,17例为良。重建所用异体骨的平均长度为64.0 mm。所有患者的后凸畸形均有改善,平均矫正角度为13.4°。在至少36个月的随访期间,未出现植入物断裂或异体骨移位情况。一期前路清创、腓骨异体骨移植并后路椎弓根螺钉内固定可提供即时稳定性、满意的对线并成功控制感染。腓骨异体骨移植似乎是前路重建的良好选择;它可实现骨融合,且避免了供区并发症。