Boucquemont Julie, Metzger Marie, Combe Christian, Stengel Bénédicte, Leffondre Karen
University of Bordeaux, ISPED, Centre INSERM U897 Epidemiology and Biostatistics, Bordeaux, France.
Inserm Unit 1018, CESP, Research Centre in Epidemiology and Population Health, Villejuif, France; University Paris-Sud 11, UMRS 1018, Villejuif, France.
PLoS One. 2014 Dec 11;9(12):e114839. doi: 10.1371/journal.pone.0114839. eCollection 2014.
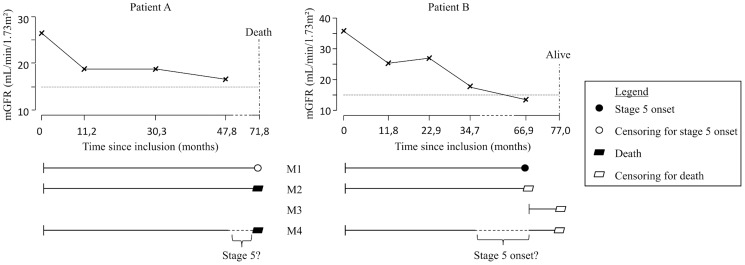
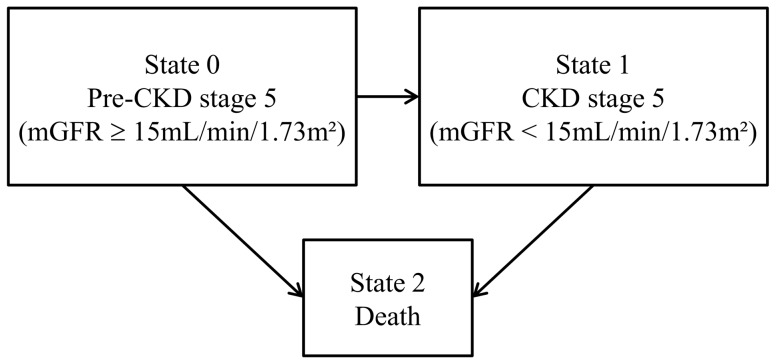
In studies investigating risk factors of chronic kidney disease (CKD) progression, one may be interested in estimating factors effects on both a fall of glomerular filtration rate (GFR) below a specific level (i.e., a CKD stage) and death. Such studies have to account for the fact that GFR is measured at intermittent visit only, which implies that progression to the stage of interest is unknown for patients who die before being observed at that stage. Our objective was to compare the results of an illness-death model that handles this uncertainty, with frequently used survival models.
This study included 1,519 patients from the NephroTest cohort with CKD stages 1-4 at baseline (69% males, 59±15 years, median protein/creatinine ratio [PCR] 27.4 mg/mmol) and subsequent annual measures of GFR (follow-up time 4.3±2.7 years). Each model was used to estimate the effects of sex, age, PCR, and GFR at baseline on the hazards of progression to CKD stage 5 (GFR<15 mL/min/1.73 m2, n = 282 observed) and death (n = 168).
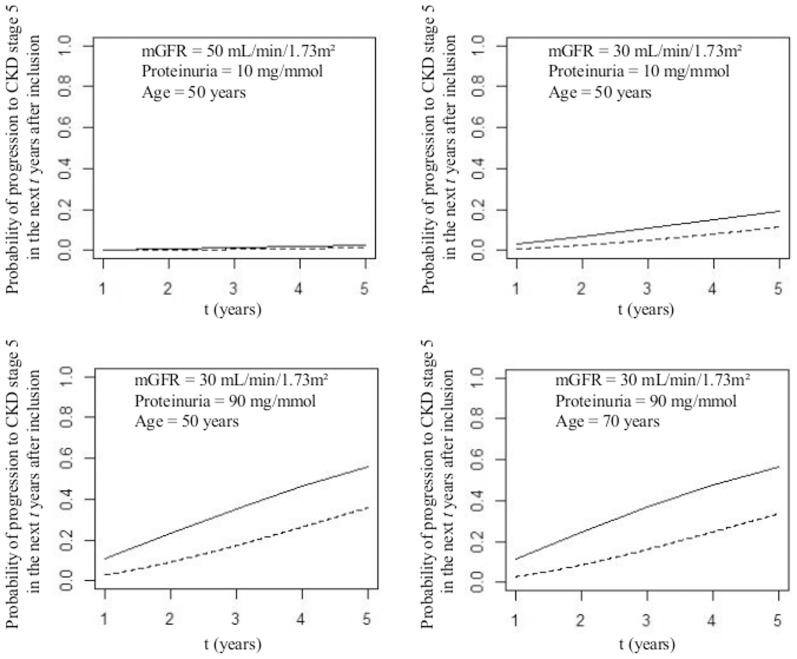
For progression to stage 5, there were only minor differences between results from the different models. The differences between results were higher for the hazard of death before or after progression. Our results also suggest that previous findings on the effect of age on end-stage renal disease are more likely due to a strong impact of age on death than to an effect on progression. The probabilities of progression were systematically under-estimated with the survival model as compared with the illness-death model.
This study illustrates the advantages of the illness-death model for accurately estimating the effects of risk factors on the hazard of progression and death, and probabilities of progression. It avoids the need to choose arbitrary time-to-event and time-to-censoring, while accounting for both interval censoring and competition by death, using a single analytical model.
在调查慢性肾脏病(CKD)进展危险因素的研究中,人们可能有兴趣估计各因素对肾小球滤过率(GFR)降至特定水平(即CKD分期)以及死亡的影响。此类研究必须考虑到GFR仅在间歇性访视时进行测量这一事实,这意味着对于在达到该分期之前就已死亡的患者,其是否进展到感兴趣的分期是未知的。我们的目标是比较处理这种不确定性的疾病 - 死亡模型与常用生存模型的结果。
本研究纳入了1519例来自NephroTest队列的患者,这些患者基线时处于CKD 1 - 4期(男性占69%,年龄59±15岁,蛋白/肌酐比值[PCR]中位数为27.4 mg/mmol),随后每年测量GFR(随访时间4.3±2.7年)。每个模型用于估计基线时性别、年龄、PCR和GFR对进展至CKD 5期(GFR<15 mL/min/1.73 m²,观察到n = 282例)和死亡(n = 168例)风险的影响。
对于进展至5期,不同模型的结果仅有微小差异。对于进展前后死亡风险,结果之间的差异更大。我们的结果还表明,先前关于年龄对终末期肾病影响的研究结果更可能是由于年龄对死亡有强烈影响,而非对进展的影响。与疾病 - 死亡模型相比,生存模型系统性地低估了进展概率。
本研究说明了疾病 - 死亡模型在准确估计危险因素对进展风险、死亡风险以及进展概率影响方面的优势。它避免了需要选择任意的事件发生时间和删失时间,同时通过单一分析模型考虑了区间删失和死亡竞争。