Gibbison Ben, Spiga Francesca, Walker Jamie J, Russell Georgina M, Stevenson Kirsty, Kershaw Yvonne, Zhao Zidong, Henley David, Angelini Gianni D, Lightman Stafford L
Department of Cardiac Anesthesia, Bristol Heart Institute, Bristol, UK.
Henry Wellcome Laboratories for Integrative Neuroscience and Endocrinology, University of Bristol, Bristol, UK.
Crit Care Med. 2015 Apr;43(4):791-800. doi: 10.1097/CCM.0000000000000773.
To characterize the dynamics of the pituitary-adrenal interaction during the course of coronary artery bypass grafting both on and off pump. Since our data pointed to a major change in adrenal responsiveness to adrenocorticotropic hormone, we used a reverse translation approach to investigate the molecular mechanisms underlying this change in a rat model of critical illness.
Prospective observational study.
Controlled experimental study.
Cardiac surgery operating rooms and critical care units.
University research laboratory.
Twenty, male patients.
Adult, male Sprague-Dawley rats.
Coronary artery bypass graft-both on and off pump.
Injection of either lipopolysaccharide or saline (controls) via a jugular vein cannula.
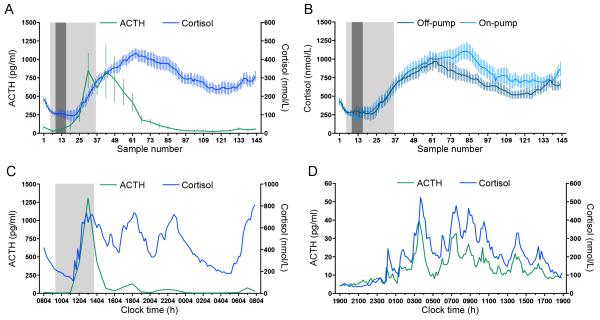
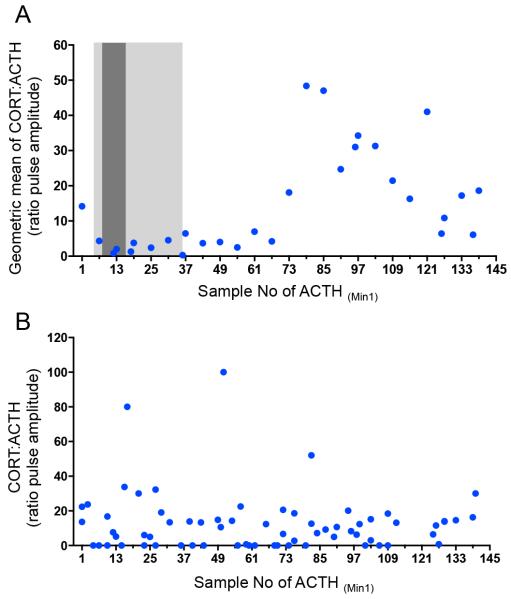
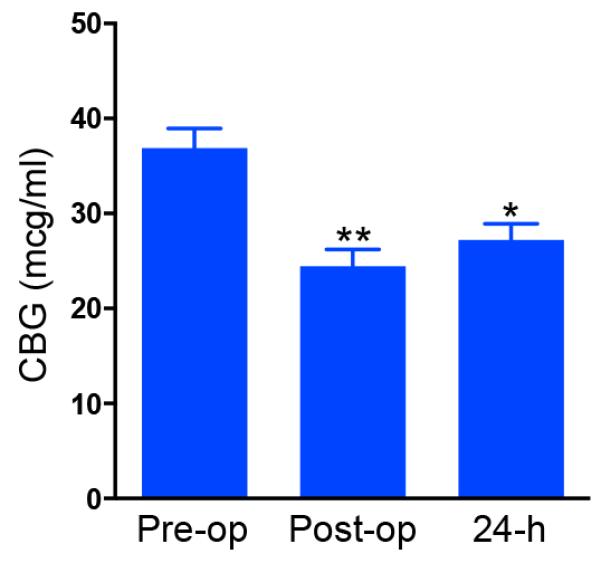
Blood samples were taken for 24 hours from placement of the first venous access. Cortisol and adrenocorticotropic hormone were measured every 10 and 60 minutes, respectively, and corticosteroid-binding globulin was measured at the beginning and end of the 24-hour period and at the end of operation. There was an initial rise in both levels of adrenocorticotropic hormone and cortisol to supranormal values at around the end of surgery. Adrenocorticotropic hormone levels then returned toward preoperative values. Ultradian pulsatility of both adrenocorticotropic hormone and cortisol was maintained throughout the perioperative period in all individuals. The sensitivity of the adrenal gland to adrenocorticotropic hormone increased markedly at around 8 hours after surgery maintaining very high levels of cortisol in the face of "basal" levels of adrenocorticotropic hormone. This sensitivity began to return toward preoperative values at the end of the 24-hour sampling period.
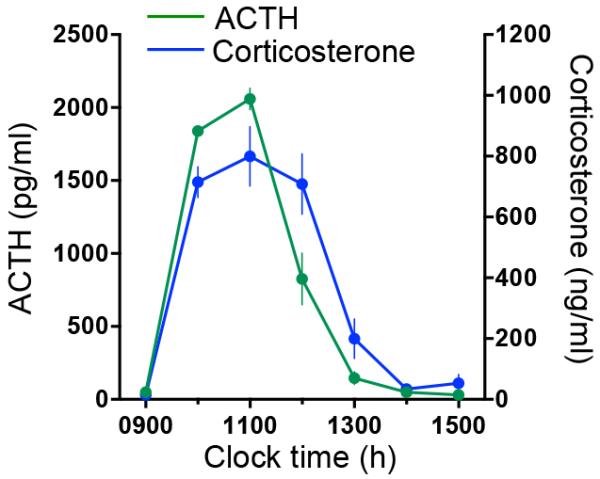
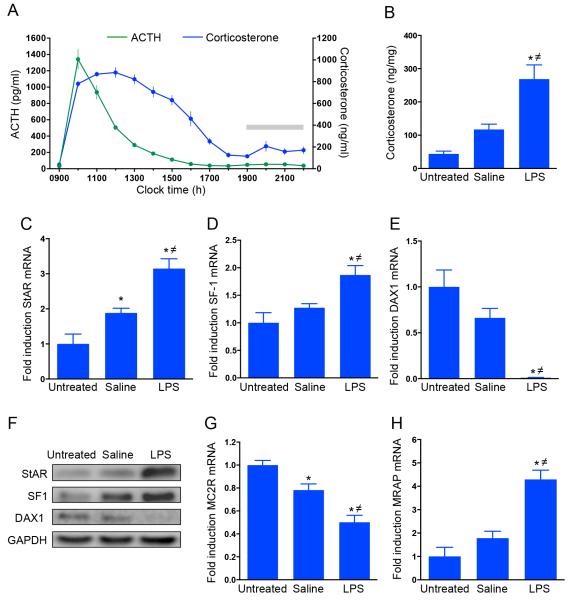
Adult, male Sprague-Dawley rats were given either lipopolysaccharide or sterile saline via a jugular vein cannula. Hourly blood samples were subsequently collected for adrenocorticotropic hormone and corticosterone measurement. Rats were killed 6 hours after the injection, and the adrenal glands were collected for measurement of steroidogenic acute regulatory protein, steroidogenic factor 1, and dosage-sensitive sex reversal, adrenal hypoplasia critical region, on chromosome X, gene 1 messenger RNAs and protein using real-time quantitative polymerase chain reaction and Western immunoblotting, respectively. Adrenal levels of the adrenocorticotropic hormone receptor (melanocortin type 2 receptor) messenger RNA and its accessory protein (melanocortin type 2 receptor accessory protein) were also measured by real-time quantitative polymerase chain reaction. In response to lipopolysaccharide, rats showed a pattern of adrenocorticotropic hormone and corticosterone that was similar to patients undergoing coronary artery bypass grafting. We were also able to demonstrate increased intra-adrenal corticosterone levels and an increase in steroidogenic acute regulatory protein, steroidogenic factor 1, and melanocortin type 2 receptor accessory protein messenger RNAs and steroidogenic acute regulatory protein, and a reduction in dosage-sensitive sex reversal, adrenal hypoplasia critical region, on chromosome X, gene 1 and melanocortin type 2 receptor messenger RNAs, 6 hours after lipopolysaccharide injection.
Severe inflammatory stimuli activate the hypothalamic-pituitary-adrenal axis resulting in increased steroidogenic activity in the adrenal cortex and an elevation of cortisol levels in the blood. Following coronary artery bypass grafting, there is a massive increase in both adrenocorticotropic hormone and cortisol secretion. Despite a subsequent fall of adrenocorticotropic hormone to basal levels, cortisol remains elevated and coordinated adrenocorticotropic hormone-cortisol pulsatility is maintained. This suggested that there is an increase in adrenal sensitivity to adrenocorticotropic hormone, which we confirmed in our animal model of immune activation of the hypothalamic-pituitary-adrenal axis. Using this model, we were able to show that this increased adrenal sensitivity results from changes in the regulation of both stimulatory and inhibitory intra-adrenal signaling pathways. Increased understanding of the dynamics of normal hypothalamic-pituitary-adrenal responses to major surgery will provide us with a more rational approach to glucocorticoid therapy in critically ill patients.
描述冠状动脉搭桥术(无论是否使用体外循环)过程中垂体 - 肾上腺相互作用的动态变化。由于我们的数据表明肾上腺对促肾上腺皮质激素的反应发生了重大变化,我们采用反向翻译方法,在危重病大鼠模型中研究这种变化的分子机制。
前瞻性观察性研究。
对照实验研究。
心脏外科手术室和重症监护病房。
大学研究实验室。
20名男性患者。
成年雄性Sprague - Dawley大鼠。
冠状动脉搭桥术(使用体外循环和不使用体外循环)。
通过颈静脉插管注射脂多糖或生理盐水(对照组)。
从首次建立静脉通路开始采集血样24小时。分别每10分钟和60分钟测量皮质醇和促肾上腺皮质激素,并在24小时期间开始和结束时以及手术结束时测量皮质类固醇结合球蛋白。在手术接近结束时,促肾上腺皮质激素和皮质醇水平均最初升高至超常值。然后促肾上腺皮质激素水平恢复到术前值。在所有个体的围手术期,促肾上腺皮质激素和皮质醇的超日波动均得以维持。肾上腺对促肾上腺皮质激素的敏感性在术后约8小时显著增加,面对“基础”水平的促肾上腺皮质激素,皮质醇维持在非常高的水平。这种敏感性在24小时采样期结束时开始恢复到术前值。
成年雄性Sprague - Dawley大鼠通过颈静脉插管给予脂多糖或无菌生理盐水。随后每小时采集血样用于测量促肾上腺皮质激素和皮质酮。注射后6小时处死大鼠,收集肾上腺用于分别使用实时定量聚合酶链反应和Western免疫印迹法测量类固醇生成急性调节蛋白、类固醇生成因子1以及位于X染色体上的剂量敏感性性别反转、肾上腺发育不全关键区域基因1的信使核糖核酸和蛋白质。还通过实时定量聚合酶链反应测量促肾上腺皮质激素受体(黑素皮质素2型受体)信使核糖核酸及其辅助蛋白(黑素皮质素2型受体辅助蛋白)的肾上腺水平。对脂多糖的反应中,大鼠表现出的促肾上腺皮质激素和皮质酮模式与接受冠状动脉搭桥术的患者相似。我们还能够证明脂多糖注射6小时后,肾上腺内皮质酮水平升高,类固醇生成急性调节蛋白、类固醇生成因子1和黑素皮质素2型受体辅助蛋白信使核糖核酸以及类固醇生成急性调节蛋白增加,而位于X染色体上的剂量敏感性性别反转、肾上腺发育不全关键区域基因1和黑素皮质素2型受体信使核糖核酸减少。
严重的炎症刺激激活下丘脑 - 垂体 - 肾上腺轴,导致肾上腺皮质类固醇生成活性增加和血液中皮质醇水平升高。冠状动脉搭桥术后,促肾上腺皮质激素和皮质醇分泌均大幅增加。尽管随后促肾上腺皮质激素降至基础水平,但皮质醇仍保持升高,并且促肾上腺皮质激素 - 皮质醇的协调性波动得以维持。这表明肾上腺对促肾上腺皮质激素的敏感性增加,我们在我们的下丘脑 - 垂体 - 肾上腺轴免疫激活动物模型中证实了这一点。使用该模型,我们能够表明这种肾上腺敏感性增加是由于肾上腺内刺激和抑制信号通路调节的变化所致。对正常下丘脑 - 垂体 - 肾上腺对大手术反应动态变化的进一步了解将为我们在危重病患者中进行糖皮质激素治疗提供更合理的方法。