Karim Nagla A, Bui Hai, Pathrose Peterson, Starnes Sandra, Patil Ninad, Shehata Mahmoud, Mostafa Ahmed, Rao Mb, Zarzour Ahmad, Anderson Marshall
Division of Hematology/Oncology, Department of Internal Medicine, University of Cincinnati, Cincinnati, OH, USA.
Department of Pathology, Cincinnati VA Medical Center, Cincinnati, OH, USA.
Clin Med Insights Oncol. 2014 Dec 7;8:139-44. doi: 10.4137/CMO.S18369. eCollection 2014.
Performance status (PS) is the only known clinical predictor of outcome in patients with advanced non-small-cell lung cancer (NSCLC), although pharmacogenomic markers may also correlate with outcome. The aim of our study was to correlate clinical and pharmacogenomic measures with overall survival.
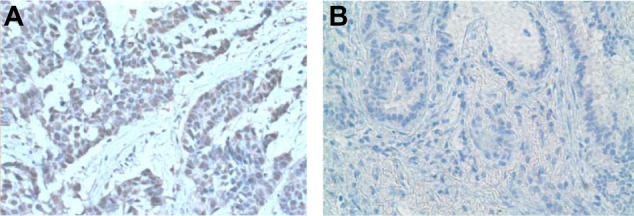
This was an IRB approved, retrospective study in which the medical records of 50 patients with advanced NSCLC from 1998-2008 were reviewed, and gender, race, PS, and chemotherapy regimens were documented. Stromal expression of pharmacogenomic markers (VEGFR, ERCC1, 14-3-3σ, pAKT, and PTEN) was measured. Clinical factors and pharmacogenomics markers were compared to overall survival using a Cox proportional hazards model.
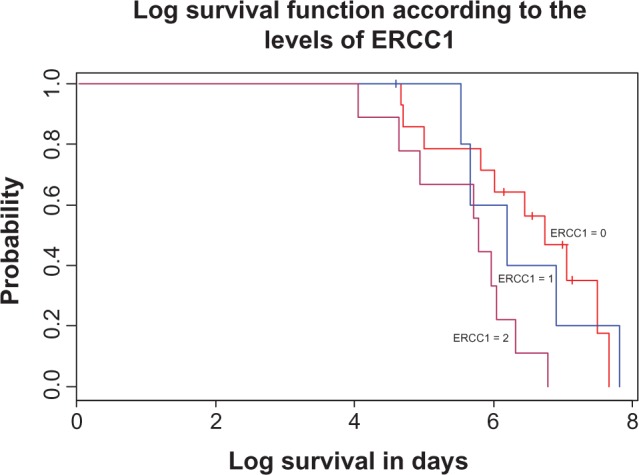
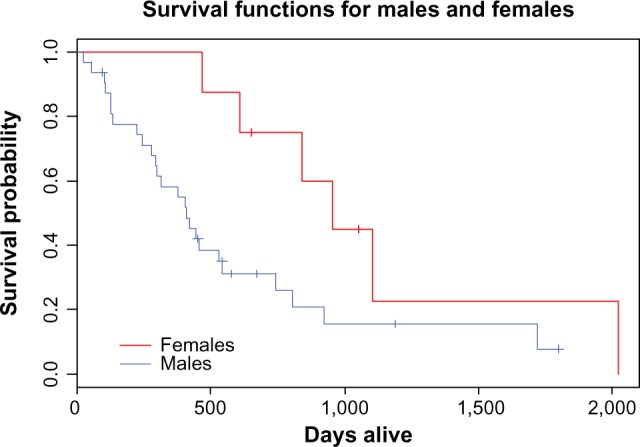
Forty patients received platinum-based therapy. Median age was 65 years. Improved PS, female gender, and gemcitabine therapy were significantly associated with longer overall survival (P = 0.004, P = 0.04, and P = 0.003, respectively). Age was not associated with survival. Caucasians had better overall survival in comparison to African Americans with median survival of 14.8 months versus 10.4 months (P = 0.1). Patients treated with platinum-based therapy had better survival of 15 months versus 8 months for non-platinum based therapy (P = 0.01). There was no significant association between any of the pharmacogenomics markers and overall survival other than in patients treated with platinum, in whom ERCC1 negativity was strongly associated with longer survival (P = 0.007).
ERCC1 negativity with platinum therapy, gemcitabine therapy, good PS, and female gender all correlated with improved overall survival in patients with advanced NSCLC.
体能状态(PS)是晚期非小细胞肺癌(NSCLC)患者已知的唯一临床预后预测指标,尽管药物基因组学标志物也可能与预后相关。我们研究的目的是将临床和药物基因组学指标与总生存期进行关联。
这是一项经机构审查委员会(IRB)批准的回顾性研究,回顾了1998年至2008年50例晚期NSCLC患者的病历,并记录了性别、种族、PS和化疗方案。测量了药物基因组学标志物(VEGFR、ERCC1、14-3-3σ、pAKT和PTEN)的基质表达。使用Cox比例风险模型将临床因素和药物基因组学标志物与总生存期进行比较。
40例患者接受了铂类治疗。中位年龄为65岁。改善的PS、女性性别和吉西他滨治疗与更长的总生存期显著相关(分别为P = 0.004、P = 0.04和P = 0.003)。年龄与生存期无关。与非裔美国人相比,白种人的总生存期更好,中位生存期分别为14.8个月和10.4个月(P = 0.1)。接受铂类治疗的患者生存期更好,铂类治疗组为15个月,非铂类治疗组为8个月(P = 0.01)。除了接受铂类治疗的患者外,任何药物基因组学标志物与总生存期均无显著关联,在接受铂类治疗的患者中,ERCC1阴性与更长的生存期密切相关(P = 0.007)。
铂类治疗时ERCC1阴性、吉西他滨治疗、良好的PS和女性性别均与晚期NSCLC患者总生存期改善相关。