Sørensen Tove, Dyb Kari, Rygh Ellen, Salvesen Rolf, Thomassen Lars
Norwegian Centre for Integrated Care and Telemedicine, PO Box 35, NO-9038, Tromsø, Norway.
Norwegian Centre for Integrated Care and Telemedicine, Kirkeveien 9, NO-4816, Kolbjørnsvik, Norway.
BMC Health Serv Res. 2014 Dec 19;14:643. doi: 10.1186/s12913-014-0643-9.
To assist small hospitals in providing advanced stroke treatment, the Norwegian Directorate of Health has recommended telemedicine services. Telestroke enables specialists to examine patients via videoconferencing supplemented by teleradiology and to provide decision support to local health care personnel. There is evidence that telestroke increases thrombolysis rates. In Norway, telemedicine has mainly been used in non-critical situations. The first telestroke trials took place in 2008. The aim of this paper is to present an overview of telestroke trials and today's status with telestroke in Norway. Based on the divergent experience from two health regions in Norway, the paper discusses crucial factors for the integration of telestroke in clinical practice.
This is a descriptive study based on multiple methods to obtain an overview of the practice and experience with telestroke in Norway. A Web and literature search for 'telestroke in Norway' was performed and compared with a survey of telemedicine services at the country's largest hospitals. These findings were supplemented by interviews with key personnel involved in telestroke in two of four health regions, as well as hospital field observations and log data of telestroke transmissions from five of the hospitals involved.
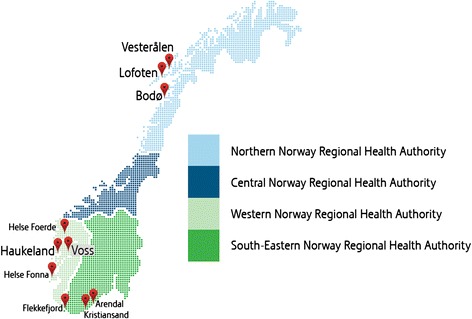
In Norway, experience in telemedicine for acute stroke care is limited. At the beginning of 2014, three of four regional health authorities were working with telestroke projects and services. Integration of the service in practice is challenging, with varying experience. The problems are not attributed to the technology in itself, but to organization (availability of staff on duty 24/7 and surveillance of the systems), motivation of staff, logistics (patient delay), and characteristics of the buildings (lack of space).
Prerequisites for successful integration of telestroke in clinical practice include realization of the collaboration potential in the technology with consistent procedures for training and triage, availability of the equipment, and providing advice beyond questions concerning thrombolysis.
为帮助小型医院提供先进的中风治疗,挪威卫生局推荐了远程医疗服务。远程中风医疗使专家能够通过视频会议并辅以远程放射学检查患者,并为当地医护人员提供决策支持。有证据表明远程中风医疗可提高溶栓率。在挪威,远程医疗主要用于非危急情况。首次远程中风医疗试验于2008年进行。本文旨在概述挪威的远程中风医疗试验及当前状况。基于挪威两个卫生区域的不同经验,本文讨论了将远程中风医疗整合到临床实践中的关键因素。
这是一项基于多种方法的描述性研究,旨在全面了解挪威远程中风医疗的实践和经验。对“挪威的远程中风医疗”进行了网络和文献搜索,并与该国最大医院的远程医疗服务调查进行了比较。通过对四个卫生区域中的两个区域参与远程中风医疗的关键人员进行访谈,以及医院实地观察和所涉五家医院的远程中风医疗传输日志数据,对这些发现进行了补充。
在挪威,急性中风护理的远程医疗经验有限。2014年初,四个区域卫生当局中有三个在开展远程中风医疗项目和服务。将该服务整合到实践中具有挑战性,经验各不相同。问题并非源于技术本身,而是源于组织(全天候值班人员的可用性和系统监控)、工作人员的积极性、后勤(患者延误)以及建筑物的特点(空间不足)。
将远程中风医疗成功整合到临床实践中的先决条件包括认识到该技术的协作潜力,具备一致的培训和分诊程序、设备可用性,并提供超出溶栓问题的建议。