Green Robert A, Hripcsak George, Salmasian Hojjat, Lazar Eliot J, Bostwick Susan B, Bakken Suzanne R, Vawdrey David K
Department of Emergency Medicine, Columbia University Medical Center and NewYork-Presbyterian Hospital, New York, NY; Division of Quality and Patient Safety, NewYork-Presbyterian Hospital, New York, NY.
Department of Biomedical Informatics, Columbia University, New York, NY; Medical Informatics Services, NewYork-Presbyterian Hospital, New York, NY.
Ann Emerg Med. 2015 Jun;65(6):679-686.e1. doi: 10.1016/j.annemergmed.2014.11.017. Epub 2014 Dec 18.
We evaluate the short- and long-term effect of a computerized provider order entry-based patient verification intervention to reduce wrong-patient orders in 5 emergency departments.
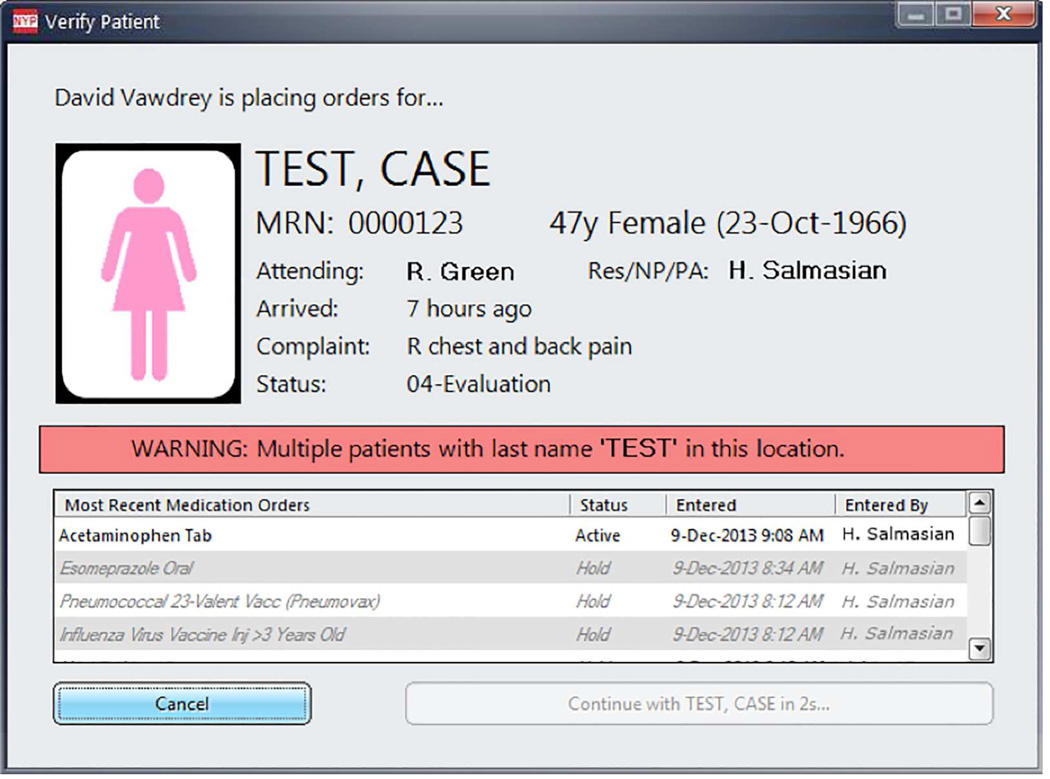
A patient verification dialog appeared at the beginning of each ordering session, requiring providers to confirm the patient's identity after a mandatory 2.5-second delay. Using the retract-and-reorder technique, we estimated the rate of wrong-patient orders before and after the implementation of the intervention to intercept these errors. We conducted a short- and long-term quasi-experimental study with both historical and parallel controls. We also measured the amount of time providers spent addressing the verification system, and reasons for discontinuing ordering sessions as a result of the intervention.
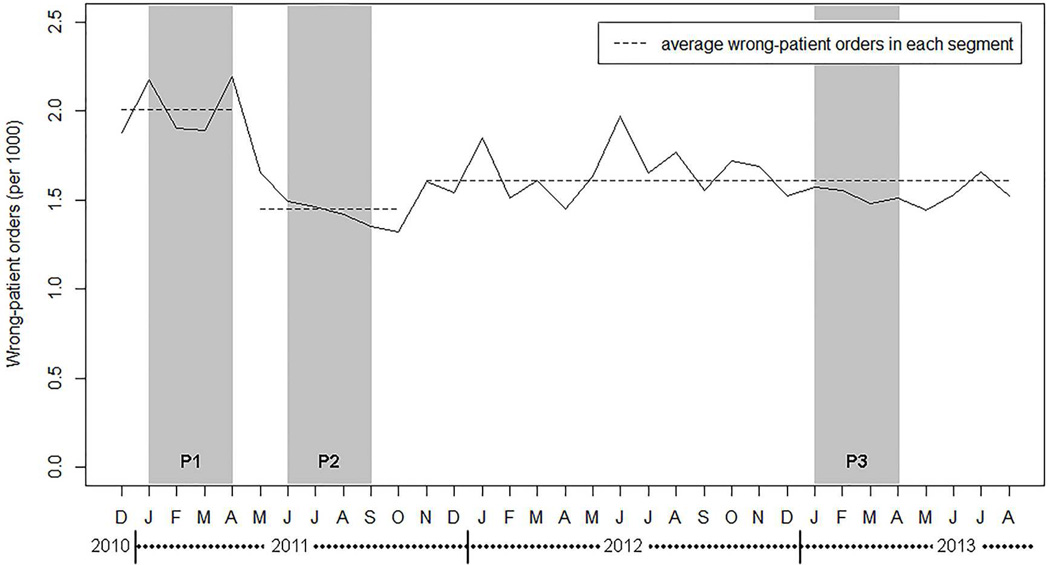
Wrong-patient orders were reduced by 30% immediately after implementation of the intervention. This reduction persisted when inpatients were used as a parallel control. After 2 years, the rate of wrong-patient orders remained 24.8% less than before intervention. The mean viewing time of the patient verification dialog was 4.2 seconds (SD=4.0 seconds) and was longer when providers indicated they placed the order for the wrong patient (4.9 versus 4.1 seconds). Although the display of each dialog took only seconds, the large number of display episodes triggered meant that the physician time to prevent each retract-and-reorder event was 1.5 hours.
A computerized provider order entry-based patient verification system led to a moderate reduction in wrong-patient orders that was sustained over time. Interception of wrong-patient orders at data entry is an important step in reducing these errors.
我们评估了一种基于计算机医嘱录入的患者验证干预措施对减少5个急诊科错发患者医嘱的短期和长期效果。
在每次开医嘱环节开始时会出现一个患者验证对话框,要求开医嘱人员在强制延迟2.5秒后确认患者身份。使用撤回并重新开医嘱技术,我们估计了干预措施实施前后错发患者医嘱的发生率,以拦截这些错误。我们进行了一项短期和长期的准实验研究,采用了历史对照和平行对照。我们还测量了开医嘱人员处理验证系统所花费的时间,以及因干预措施而中断开医嘱环节的原因。
干预措施实施后,错发患者医嘱立即减少了30%。当将住院患者作为平行对照时,这种减少持续存在。2年后,错发患者医嘱的发生率仍比干预前低24.8%。患者验证对话框的平均查看时间为4.2秒(标准差=4.0秒),当开医嘱人员表示他们为错误的患者开了医嘱时,查看时间更长(4.9秒对4.1秒)。尽管每个对话框的显示仅需几秒钟,但大量的显示事件意味着医生为防止每次撤回并重新开医嘱事件所花费的时间为1.5小时。
基于计算机医嘱录入的患者验证系统使错发患者医嘱适度减少,并随着时间的推移得以持续。在数据录入时拦截错发患者医嘱是减少这些错误的重要一步。