Suzuki Akio, Kobayashi Ryo, Okayasu Shinji, Kuze Bunya, Aoki Mitsuhiro, Mizuta Keisuke, Itoh Yoshinori
Department of Pharmacy, Gifu University Hospital, Gifu, Japan.
Department of Otolaryngology, Gifu University Graduate School of Medicine, Gifu, Japan.
PLoS One. 2014 Dec 30;9(12):e115879. doi: 10.1371/journal.pone.0115879. eCollection 2014.
To determine whether adverse events extend the duration of hospitalization, and to evaluate the effectiveness of medical intervention in ameliorating adverse events and reducing the prolonged hospital stay associated with adverse events.
A single arm intervention study was conducted from October 2012 to March 2014 in the otolaryngology ward of a 614-bed, university-affiliated hospital. Adverse events were monitored daily by physicians, pharmacists and nurses, and recorded in the electronic medical chart for each patient. Appropriate drug management of adverse events was performed by physicians in liaison with pharmacists. The Kaplan-Meier method was used to assess the length of hospitalization of patients who underwent medical intervention for adverse events.
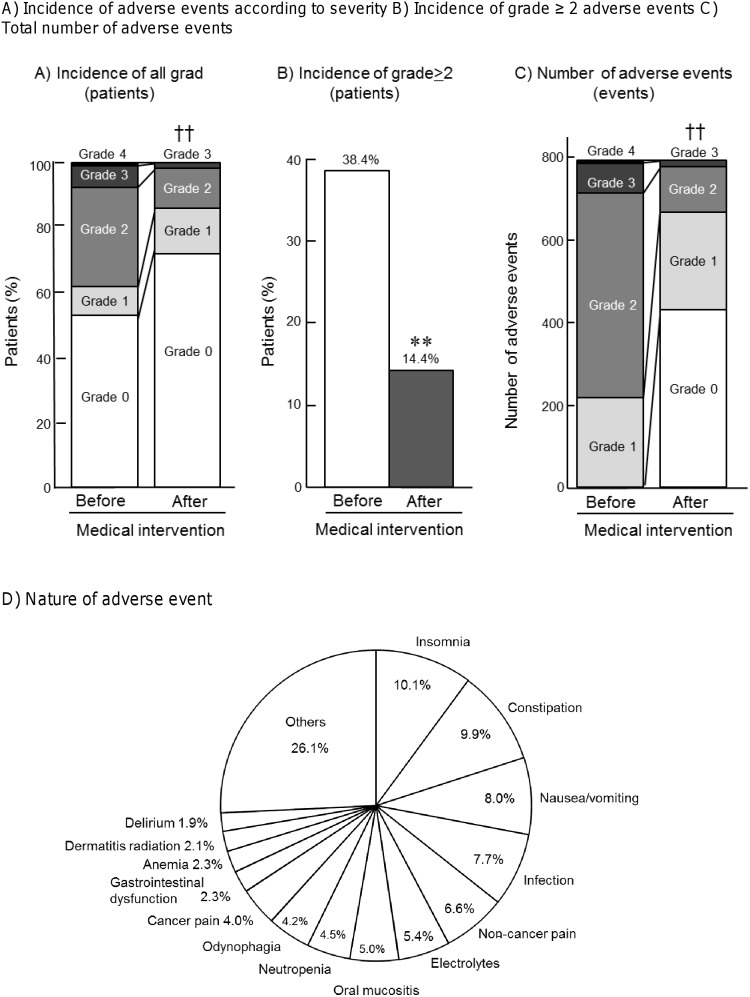
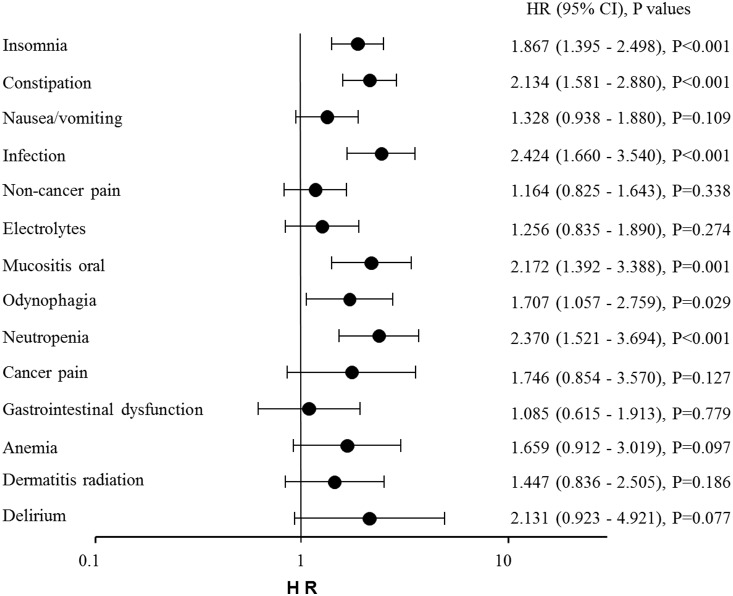
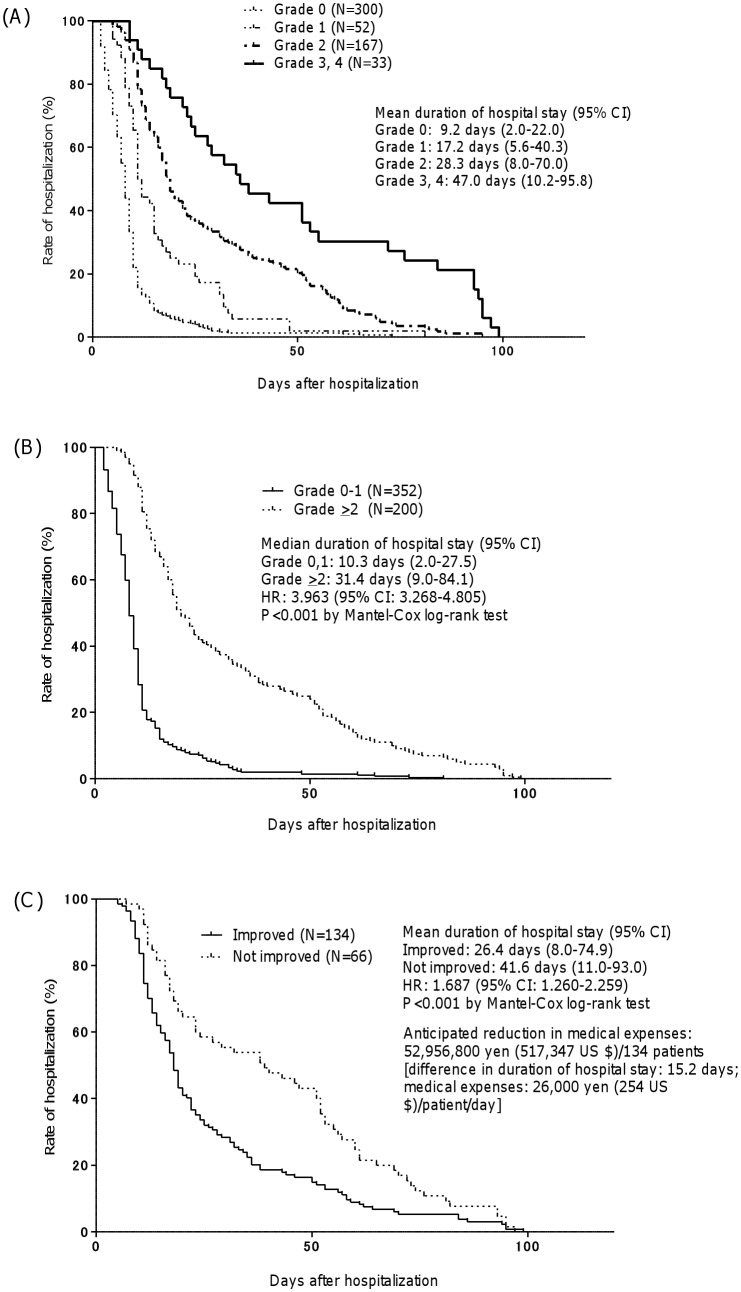
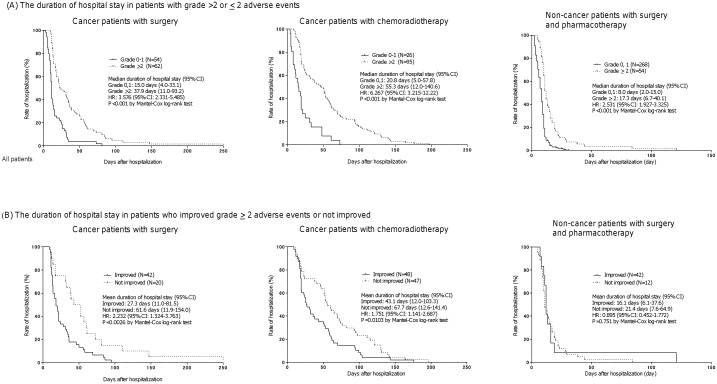
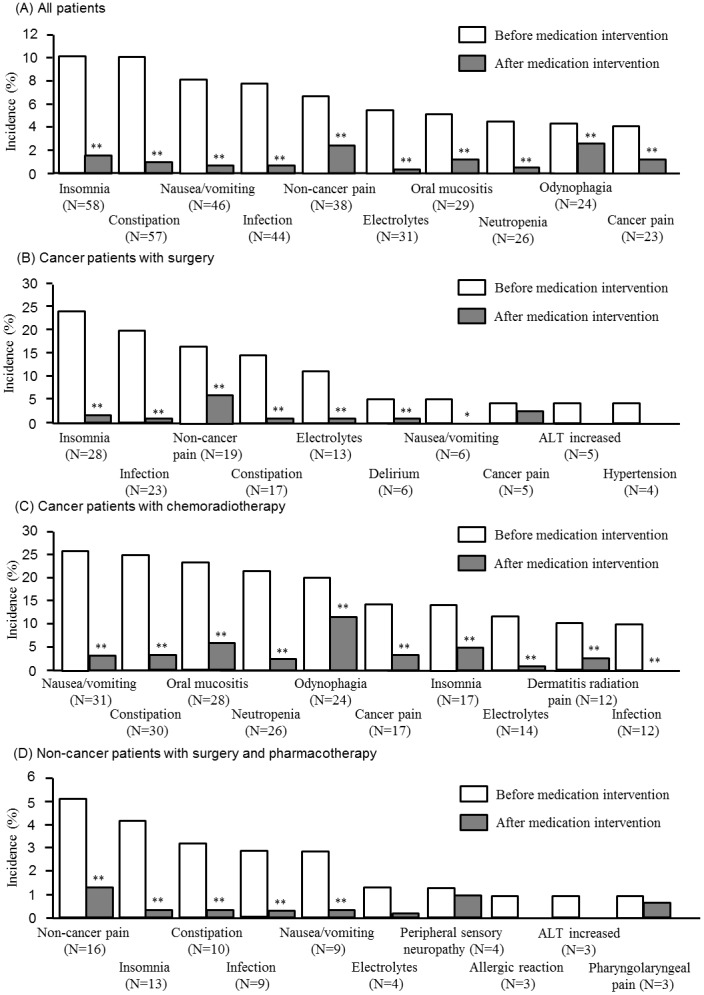
Of 571 patients admitted to the otolaryngology ward in a year, 219 patients (38.4%) experienced adverse events of grade ≥2. The duration of hospitalization was affected by the grade of adverse events, with a mean duration of hospital stay of 9.2, 17.2, 28.3 and 47.0 days for grades 0, 1, 2, and 3-4, respectively. Medical intervention lowered the incidence of grade ≥2 adverse events to 14.5%. The length of hospitalization was significantly shorter in patients who showed an improvement of adverse events after medical intervention than those who did not (26.4 days vs. 41.6 days, hazard ratio 1.687, 95% confidence interval: 1.260-2.259, P<0.001). A multivariate Cox proportional hazard analysis indicated that insomnia, constipation, nausea/vomiting, infection, non-cancer pain, oral mucositis, odynophagia and neutropenia were significant risk factors for prolongation of hospital stay.
Patients who experienced adverse events are at high risk of prolonged hospitalization. Medical intervention for adverse events was found to be effective in reducing the length of hospital stay associated with adverse events.
确定不良事件是否会延长住院时间,并评估医疗干预在改善不良事件及减少与不良事件相关的延长住院时间方面的有效性。
2012年10月至2014年3月,在一所拥有614张床位的大学附属医院的耳鼻喉科病房进行了一项单臂干预研究。医生、药剂师和护士每天监测不良事件,并记录在每位患者的电子病历中。医生与药剂师联合对不良事件进行适当的药物管理。采用Kaplan-Meier方法评估因不良事件接受医疗干预的患者的住院时间。
一年中入住耳鼻喉科病房的571例患者中,219例(38.4%)发生了≥2级不良事件。住院时间受不良事件分级的影响,0级、1级、2级和3 - 4级患者的平均住院时间分别为9.2天、17.2天、28.3天和47.0天。医疗干预使≥2级不良事件的发生率降至14.5%。医疗干预后不良事件有所改善的患者的住院时间明显短于未改善的患者(26.4天对41.6天,风险比1.687,95%置信区间:1.260 - 2.259,P<0.001)。多因素Cox比例风险分析表明,失眠、便秘、恶心/呕吐、感染、非癌性疼痛、口腔黏膜炎、吞咽痛和中性粒细胞减少是延长住院时间的显著危险因素。
发生不良事件的患者住院时间延长的风险较高。发现针对不良事件的医疗干预在减少与不良事件相关的住院时间方面是有效的。