Patnaik M M, Wassie E A, Padron E, Onida F, Itzykson R, Lasho T L, Kosmider O, Finke C M, Hanson C A, Ketterling R P, Komrokji R, Tefferi A, Solary E
Department of Medicine, Division of Hematology, Mayo Clinic, Rochester, MN, USA.
Malignant Hematology and Immunology Program, H. Lee Moffitt Cancer Center, Tampa, FL, USA.
Blood Cancer J. 2015 Jan 2;5(1):e270. doi: 10.1038/bcj.2014.90.
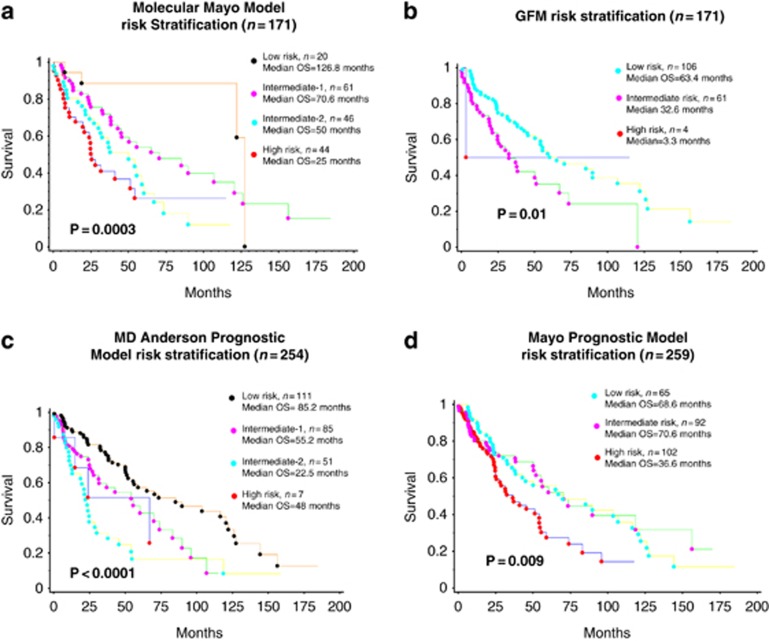
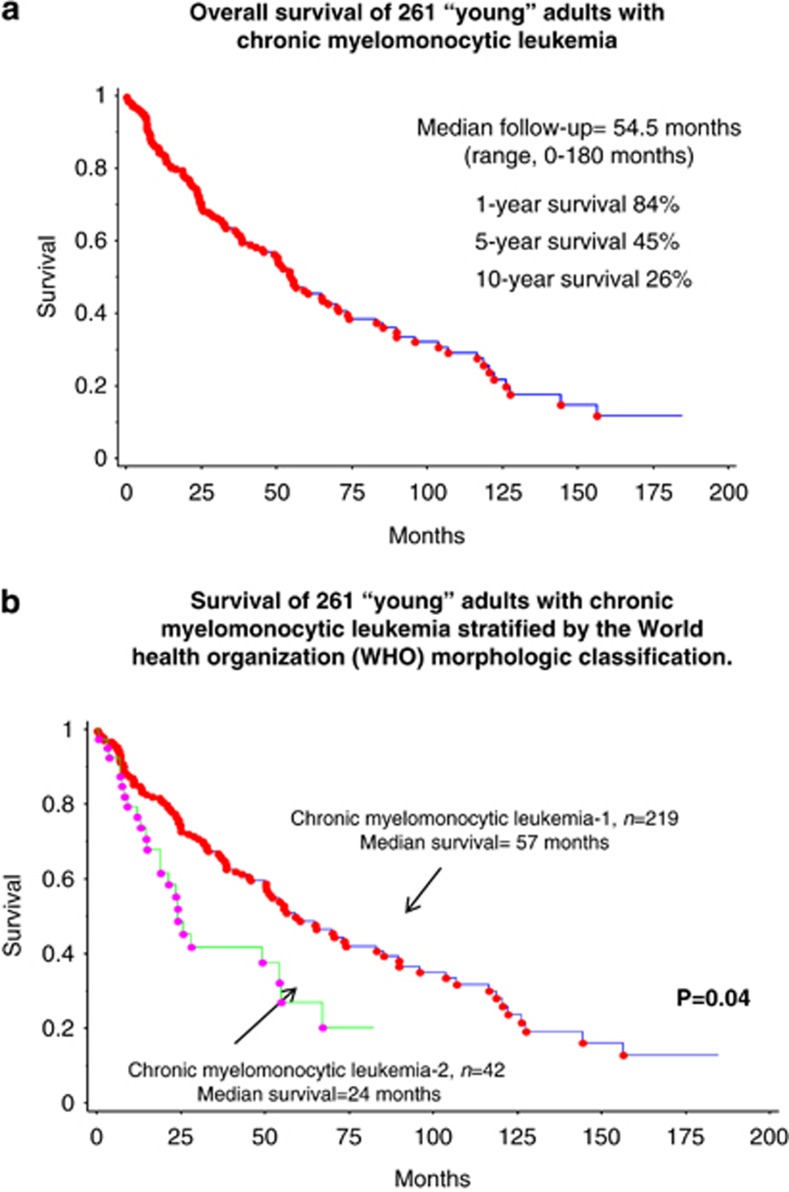
In patients with chronic myelomonocytic leukemia (CMML), age>65 years is an adverse prognostic factor. Our objective in the current study was to examine risk factors for survival and treatment outcome in 261 'young' adults with CMML, as defined by age ⩽65 years. In multivariable analysis, lower HB (P=0.01), higher circulating blast % (P=0.002), ASXL1 (P=0.0007) and SRSF2 mutations (P=0.008) and Mayo-French cytogenetic stratification (P=0.04) negatively impacted survival. Similarly, leukemia-free survival was independently affected by higher circulating blast % (P<0.0001), higher bone marrow blast % (P=0.0007) and the presence of circulating immature myeloid cells (P=0.0002). Seventy-five (29%) patients received hypomethylating agents (HMA), with the median number of cycles being 5, and the median duration of therapy being 5 months. The over-all response rate was 40% for azacitidine and 30% for decitabine. Fifty-three (24%) patients underwent an allogeneic hematopoietic stem cell transplant (AHSCT), with a response rate of 56% and a non-relapse mortality of 19%. Survival in young adults with CMML, although higher than in older patients, is poor and even worse in the presence of ASXL1 and SRSF2 mutations. Treatment outcome was more impressive with AHSCT than with HMA and neither was influenced by ASXL1/SRSF2 mutations or karyotype.
在慢性粒单核细胞白血病(CMML)患者中,年龄>65岁是一个不良预后因素。我们在本研究中的目的是检查261名年龄≤65岁的“年轻”CMML成年患者的生存和治疗结果的危险因素。在多变量分析中,较低的血红蛋白(HB)(P=0.01)、较高的循环原始细胞百分比(P=0.002)、ASXL1(P=0.0007)和SRSF2突变(P=0.008)以及梅奥-法国细胞遗传学分层(P=0.04)对生存产生负面影响。同样,无白血病生存期独立地受到较高的循环原始细胞百分比(P<0.0001)、较高的骨髓原始细胞百分比(P=0.0007)和循环未成熟髓样细胞的存在(P=0.0002)的影响。75名(29%)患者接受了去甲基化药物(HMA)治疗,中位疗程数为5个,中位治疗持续时间为5个月。阿扎胞苷的总体缓解率为40%,地西他滨为30%。53名(24%)患者接受了异基因造血干细胞移植(AHSCT),缓解率为56%,非复发死亡率为19%。CMML年轻成人患者的生存率虽然高于老年患者,但仍然较差,在存在ASXL1和SRSF2突变的情况下更差。AHSCT的治疗结果比HMA更令人印象深刻,且两者均不受ASXL1/SRSF2突变或核型的影响。