Têtu Bernard, Perron Émilie, Louahlia Said, Paré Guy, Trudel Marie-Claude, Meyer Julien
Diagn Pathol. 2014;9 Suppl 1(Suppl 1):S1. doi: 10.1186/1746-1596-9-S1-S1. Epub 2014 Dec 19.
The Eastern Quebec Telepathology Network (called Réseau de Télépathologie de l'Est du Québec in French) was created to provide uniform diagnostic telepathology services in a huge territory with low population density. We report our first 3-year experience.
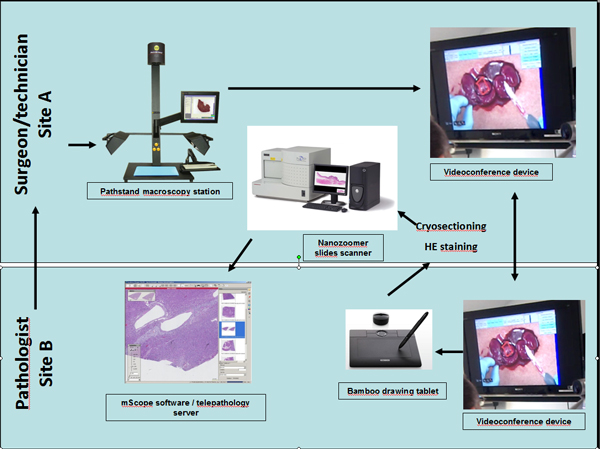
The network was funded equally by the Québec ministry of Health and Canada Health Infoway, a federal telehealth funding agency. The coverage includes intraoperative consultations (IOC), expert opinions, urgent analyses and supervision of macroscopic description. The deployment of the equipment and software started in 2010 and clinical activities began in January 2011. This network comprises 24 hospitals providing oncologic surgery, of which 7 have no pathology laboratory and 4 have a pathology laboratory but no pathologist. The real-time gross evaluation during IOC was performed using a macroscopy station and the sample selection was performed distantly by a technician, a pathology assistant or the surgeon under on-site pathologist supervision. Slides were scanned into whole-slide images (WSI).
As per March 2014, 7,440 slides had been scanned for primary/urgent diagnosis; 1,329 for IOC cases and 2,308 for expert opinions. A 98% concordance rate was found for IOC compared to paraffin material and the average turnaround time was 20 minutes. Expert opinion reports were signed out within 24 hours in 68% of cases and within 72 hours in 85%. A recent multi-method evaluation study of the Network demonstrated that, thanks to telepathology: 1. interruption of IOC service was prevented in hospitals with no pathologist on site; 2. two-stage surgeries and patients transfers were prevented according to surgeons and pathologists; 3. retention and recruitment of surgeons in remote hospitals were facilitated; and 4. professional isolation among pathologists working alone was reduced. This study also demonstrated that wider adoption of telepathology would require technological improvement and that the sustainability of the network requires better coordination and the development of a supra-regional pathology organisation.
The Eastern Quebec Telepathology Network allowed the maintenance of rapid and high quality pathology services in more than 20 sites disseminated on a huge territory. A second phase is underway to expand telepathology to other regions across the province.
魁北克东部远程病理学网络(法语称为Réseau de Télépathologie de l'Est du Québec)的创建是为了在人口密度低的广大地区提供统一的诊断远程病理学服务。我们报告我们最初三年的经验。
该网络由魁北克卫生部和加拿大健康信息高速公路(一个联邦远程医疗资助机构)平均出资。其覆盖范围包括术中会诊(IOC)、专家意见、紧急分析以及大体描述的监督。设备和软件的部署于2010年开始,临床活动于2011年1月启动。该网络由24家提供肿瘤外科手术的医院组成,其中7家没有病理实验室,4家有病理实验室但没有病理学家。术中会诊期间的实时大体评估使用一个大体检查工作站进行,样本选择由技术员、病理助理或外科医生在现场病理学家的监督下远程完成。玻片被扫描成全玻片图像(WSI)。
截至2014年3月,已扫描7440张玻片用于初步/紧急诊断;1329张用于术中会诊病例,2308张用于专家意见。术中会诊与石蜡材料相比的符合率为98%,平均周转时间为20分钟。68%的专家意见报告在24小时内发出,85%在72小时内发出。最近对该网络的一项多方法评估研究表明,得益于远程病理学:1. 在没有现场病理学家的医院中防止了术中会诊服务的中断;2. 根据外科医生和病理学家的说法,避免了两阶段手术和患者转运;3. 促进了偏远医院外科医生的留用和招聘;4. 减少了独自工作的病理学家之间的职业隔离。这项研究还表明,更广泛地采用远程病理学将需要技术改进,并且该网络的可持续性需要更好的协调以及建立一个超区域病理组织。
魁北克东部远程病理学网络使得在分布于广大地区的20多个地点维持了快速且高质量的病理学服务。第二阶段正在进行中,以将远程病理学扩展到全省其他地区。