Blandizzi Corrado, Viscomi Giuseppe Claudio, Scarpignato Carmelo
Division of Pharmacology and Chemotherapy, Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Research and Development Division, Alfa Wassermann SpA, Bologna, Italy.
Drug Des Devel Ther. 2014 Dec 16;9:1-11. doi: 10.2147/DDDT.S72572. eCollection 2015.
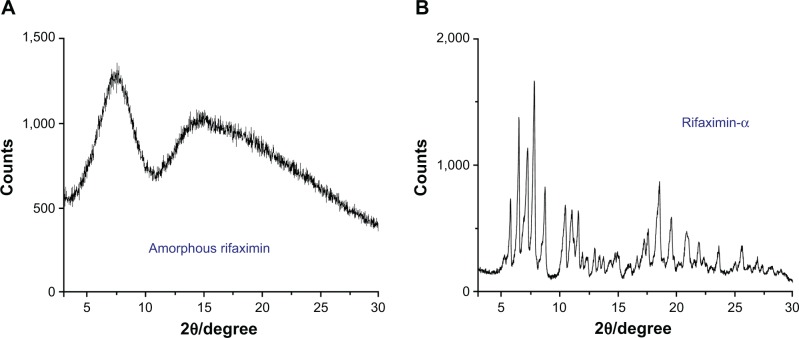
Rifaximin is an antibiotic, acting locally in the gastrointestinal tract, which may exist in different crystal as well as amorphous forms. The current marketed rifaximin formulation contains polymorph alpha, the systemic bioavailability of which is very limited. This study compared the pharmacokinetics of this formulation with those of the amorphous form.
Amorphous rifaximin was specifically prepared for the study and formulated as the marketed product. Two doses (200 mg and 400 mg) of both formulations were given to two groups of 12 healthy volunteers of either sex according to a single-blind, randomized, two-treatment, single-dose, two-period, cross-over design. Plasma and urine samples were collected at preset times (for 24 hours or 48 hours, respectively) after dosing, and assayed for rifaximin concentrations by high-performance liquid chromatography-mass spectrometry.
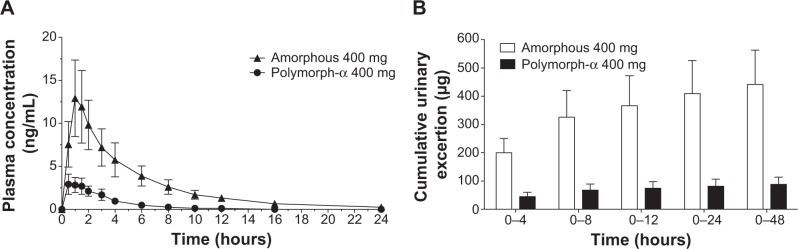
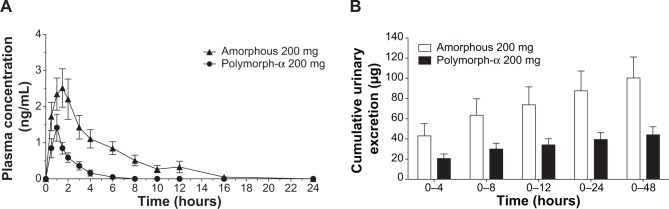
For both dose levels, peak plasma concentration, area under the concentration-time curve, and cumulative urinary excretion were significantly higher after administration of amorphous rifaximin than rifaximin-α. Ninety percent confidence intervals for peak plasma concentration, area under the concentration-time curve, and urinary excretion ratios were largely outside the upper limit of the accepted (0.80-1.25) range, indicating higher systemic bioavailability of the amorphous rifaximin. The few adverse events recorded were not serious and not related to the study medications.
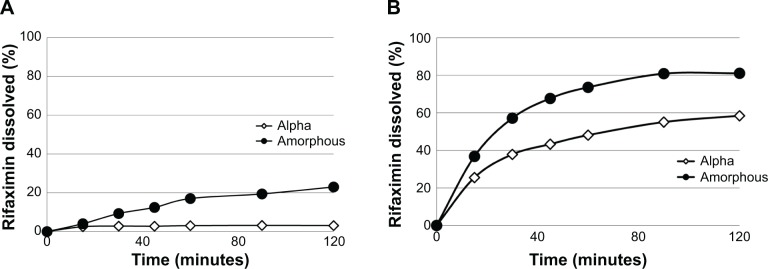
Rifaximin-α, a crystal polymorph, does differ from the amorphous form, the latter being systemically more bioavailable. In this regard, care must be taken when using - as a medicinal product - a formulation containing even small amounts of amorphous form, which may alter the peculiar pharmacologic properties of this poorly absorbed antibiotic.
利福昔明是一种抗生素,在胃肠道局部起作用,可能以不同的晶体以及无定形形式存在。目前市售的利福昔明制剂含有α多晶型物,其全身生物利用度非常有限。本研究比较了该制剂与无定形形式的药代动力学。
专门制备了无定形利福昔明用于本研究,并将其制成市售产品的剂型。按照单盲、随机、双治疗、单剂量、两周期、交叉设计,将两种制剂的两个剂量(200毫克和400毫克)给予两组各12名男女健康志愿者。给药后在预设时间(分别为24小时或48小时)采集血浆和尿液样本,并用高效液相色谱 - 质谱法测定利福昔明浓度。
对于两个剂量水平,给予无定形利福昔明后,血浆峰浓度、浓度 - 时间曲线下面积和累积尿排泄量均显著高于利福昔明α。血浆峰浓度、浓度 - 时间曲线下面积和尿排泄率的90%置信区间大多超出公认范围(0.80 - 1.25)的上限,表明无定形利福昔明的全身生物利用度更高。记录到的少数不良事件不严重,且与研究药物无关。
晶体多晶型物利福昔明α与无定形形式确实不同,后者的全身生物利用度更高。在这方面,当使用含有即使少量无定形形式的制剂作为药品时必须谨慎,因为这可能会改变这种吸收不良的抗生素的特殊药理特性。