Kolek Matthew J, Muehlschlegel J Daniel, Bush William S, Parvez Babar, Murray Katherine T, Stein C Michael, Shoemaker M Benjamin, Blair Marcia A, Kor Kaylen C, Roden Dan M, Donahue Brian S, Fox Amanda A, Shernan Stanton K, Collard Charles D, Body Simon C, Darbar Dawood
Department of Medicine, Vanderbilt University, Nashville, TN.
Department of Anesthesiology, Perioperative & Pain Medicine, Brigham and Women's Hospital, Harvard University, Boston, MA.
Circ Arrhythm Electrophysiol. 2015 Feb;8(1):25-31. doi: 10.1161/CIRCEP.114.002300. Epub 2015 Jan 7.
Postoperative atrial fibrillation (PoAF) is common after coronary artery bypass grafting. We previously showed that atrial fibrillation susceptibility single nucleotide polymorphisms (SNPs) at the chromosome 4q25 locus are associated with PoAF. Here, we tested the hypothesis that a combined clinical and genetic model incorporating atrial fibrillation risk SNPs would be superior to a clinical-only model.
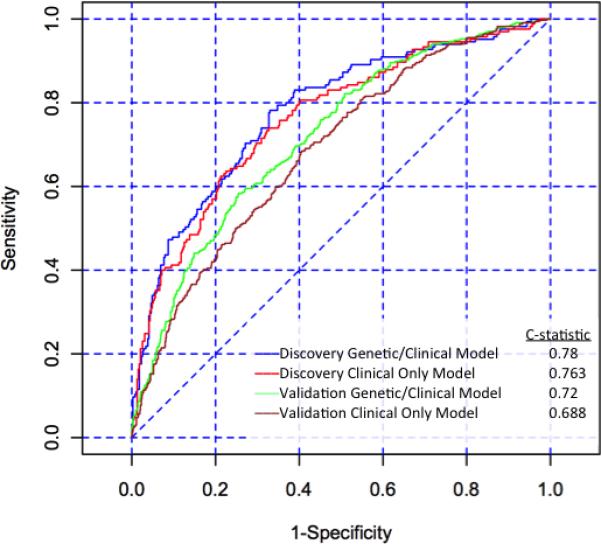
We developed and externally validated clinical and clinical/genetic risk models for PoAF. The discovery and validation cohorts included 556 and 1164 patients, respectively. Clinical variables previously associated with PoAF and 13 SNPs at loci associated with atrial fibrillation in genome-wide association studies were considered. PoAF occurred in 30% and 29% of patients in the discovery and validation cohorts, respectively. In the discovery cohort, a logistic regression model with clinical factors had good discrimination, with an area under the receiver operator characteristic curve of 0.76. The addition of 10 SNPs to the clinical model did not improve discrimination (area under receiver operator characteristic curve, 0.78; P=0.14 for difference between the 2 models). In the validation cohort, the clinical model had good discrimination (area under the receiver operator characteristic curve, 0.69) and addition of genetic variables resulted in a marginal improvement in discrimination (area under receiver operator characteristic curve, 0.72; P<0.0001).
We developed and validated a model for the prediction of PoAF containing common clinical variables. Addition of atrial fibrillation susceptibility SNPs did not improve model performance. Tools to accurately predict PoAF are needed to risk stratify patients undergoing coronary artery bypass grafting and identify candidates for prophylactic therapies.
冠状动脉旁路移植术后,术后房颤(PoAF)很常见。我们之前表明,4号染色体q25位点的房颤易感性单核苷酸多态性(SNP)与PoAF相关。在此,我们检验了一个假设,即结合房颤风险SNP的临床和遗传联合模型将优于仅基于临床因素的模型。
我们开发并外部验证了PoAF的临床及临床/遗传风险模型。发现队列和验证队列分别包括556例和1164例患者。考虑了先前与PoAF相关的临床变量以及全基因组关联研究中与房颤相关位点的13个SNP。发现队列和验证队列中分别有30%和29%的患者发生PoAF。在发现队列中,包含临床因素的逻辑回归模型具有良好的区分度,受试者操作特征曲线下面积为0.76。在临床模型中加入10个SNP并未改善区分度(受试者操作特征曲线下面积,0.78;两个模型之间差异的P值为0.14)。在验证队列中,临床模型具有良好的区分度(受试者操作特征曲线下面积,0.69),加入遗传变量后区分度有轻微改善(受试者操作特征曲线下面积,0.72;P<0.0001)。
我们开发并验证了一个用于预测PoAF的模型,该模型包含常见临床变量。加入房颤易感性SNP并未改善模型性能。需要准确预测PoAF的工具来对接受冠状动脉旁路移植术的患者进行风险分层,并识别预防性治疗的候选者。