Manabe Yukari C, Namale Gertrude, Nalintya Elizabeth, Sempa Joseph, Ratanshi Rosalind Parkes, Pakker Nadine, Katabira Elly
Infectious Diseases Institute, Makerere College of Health Sciences, PO Box 22418, Mulago Hospital Complex, Kampala, Uganda.
Division of Infectious Diseases, Department of Medicine, Johns Hopkins University, Baltimore, MD, USA.
BMC Infect Dis. 2015 Jan 13;15:15. doi: 10.1186/s12879-014-0739-1.
Syphilis infection during pregnancy leads to avoidable morbidity and mortality and remains a significant problem in sub-Saharan Africa. Despite global initiatives to increase the proportion of pregnant women screened, implementation has been slow. We sought to investigate the feasibility of adding syphilis screening within an integrated antenatal HIV clinic.
Pregnant women attending the HIV antenatal clinic were sequentially enrolled and consenting participants answered a questionnaire on sexual behavior and previous pregnancies, provided sociodemographic data, and were tested using rapid plasmin reagin (RPR). If positive, participants were treated with benzathine penicillin. All were given a partner notification slip and were followed up after delivery to determine birth outcomes.
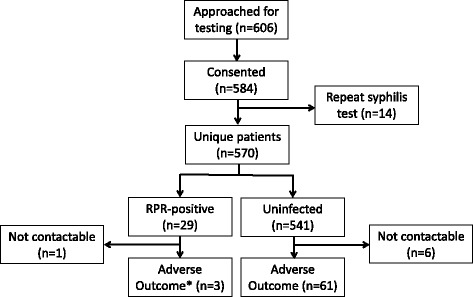
584 of 606 (95.7%) women approached and consented to test for syphilis. 570 women were enrolled (median age 29 (IQR 25-32) with a median (IQR) CD4 of 372 (257-569) cells/μL). Of the 5.1% (29/570) with a positive RPR, all were asymptomatic, were successfully contacted, and treated with benzathine penicillin without adverse reactions. Overall, 61 (12.1%) of the participants had an adverse birth outcome. In the bivariate analysis, only age was significantly different between those with and without a positive RPR (RR = 1.15, 95% CI 1.065-1.248; p < 0.001). Partners of only 10 (34.5%) participants returned for treatment.
Structural interventions such as opt-out testing for syphilis within integrated HIV-antenatal care clinics are feasible and capitalize on the excellent care programs that have already been established for HIV care. Novel approaches are required for partner notification.
孕期梅毒感染会导致可避免的发病和死亡,在撒哈拉以南非洲仍然是一个重大问题。尽管全球采取了各项举措来提高接受筛查的孕妇比例,但实施进展缓慢。我们试图调查在综合产前艾滋病毒诊所增加梅毒筛查的可行性。
依次纳入到艾滋病毒产前诊所就诊的孕妇,同意参与的受试者回答了关于性行为和既往妊娠的问卷,提供了社会人口学数据,并采用快速血浆反应素环状卡片试验(RPR)进行检测。如果结果呈阳性,受试者接受苄星青霉素治疗。所有受试者均收到一份性伴侣通知单,并在分娩后接受随访以确定分娩结局。
606名女性中,有584名(95.7%)同意接受梅毒检测。共纳入570名女性(中位年龄29岁(四分位间距25 - 32岁),CD4细胞计数中位值(四分位间距)为372(257 - 569)个/μL)。在RPR检测呈阳性的5.1%(29/570)受试者中,所有人均无症状,均成功联系到并接受了苄星青霉素治疗,且未出现不良反应。总体而言,61名(12.1%)受试者出现了不良分娩结局。在双变量分析中,RPR检测阳性者与阴性者之间只有年龄存在显著差异(相对危险度 = 1.15,95%置信区间1.065 - 1.248;p < 0.001)。只有10名(34.5%)受试者的性伴侣返回接受治疗。
在综合艾滋病毒产前护理诊所开展梅毒不记名检测等结构性干预措施是可行的,并且利用了已建立的出色的艾滋病毒护理项目。性伴侣通知需要采用新方法。