Servie de Réanimation Polyvalente, Centre de Réanimation, Hôpital Roger Salengro, CHRU, 2 Avenue Oscar Lambret, Lille Cedex 59037, France.
Service d'Anesthésie Obstétricale, Hôpital Jeanne de Flandre, CHRU, 2 Avenue Oscar Lambret, Lille Cedex 59037, France.
Ann Intensive Care. 2014 Nov 25;4:36. doi: 10.1186/s13613-014-0036-6. eCollection 2014.
Even in developed countries, severe specific pregnancy complications may occur in the immediate postpartum period and require admission to the ICU. The characteristics and risk factors of acute renal failure (ARF) induced by these complications and their treatments are not well known.
We performed a retrospective multicenter study in three intensive care departments linked to level III maternity wards in the north of France. All patients admitted to ICU for postpartum complications over a 5-year period (2008 to 2012) were included. Clinical and biological data, delivery characteristics, type of complications, and treatments were compared by univariate and multivariate analyses according to the occurrence and severity of ARF.
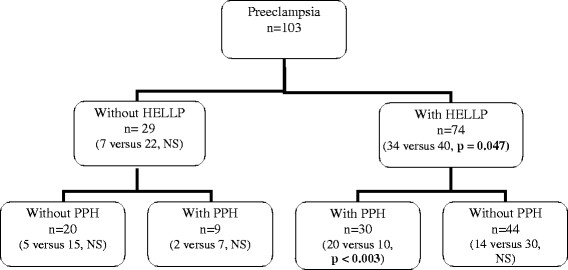
One hundred eighty-two patients admitted to ICU for postpartum complications were included in the study. Sixty-eight patients (37%) developed an ARF: 49 with a low or medium severity and 19 with a severe ARF requiring renal replacement therapy. Hemolysis, elevated liver enzyme, and low platelet count (HELLP) syndrome on its own (p = 0.047) or combined with postpartum haemorrhage (p = 0.003), previous treatment by hyperoncotic albumin infusion (p = 0.001) and blockade of fibrinolysis by tranexamic acid (p = 0.03), was associated with secondary ARF. By multivariate analysis, the only independent factors were the association of HELLP syndrome with postpartum haemorrhage and the use of hyperoncotic albumin infusion.
HELLP syndrome associated with postpartum haemorrhage induces a high risk of ARF in the complicated postpartum setting. A particular attention should be given to treatments that could worsen the kidney function in that situation.
即使在发达国家,严重的特定妊娠并发症也可能在产后立即发生,并需要入住 ICU。这些并发症引起的急性肾衰竭(ARF)的特征和危险因素及其治疗方法尚不清楚。
我们在法国北部的三个与三级产科病房相关的重症监护病房进行了一项回顾性多中心研究。纳入了在 5 年内(2008 年至 2012 年)因产后并发症而入住 ICU 的所有患者。根据 ARF 的发生和严重程度,通过单变量和多变量分析比较了临床和生物学数据、分娩特征、并发症类型和治疗方法。
研究纳入了 182 例因产后并发症而入住 ICU 的患者。68 例(37%)发生 ARF:49 例为低或中度严重程度,19 例为需要肾脏替代治疗的严重 ARF。单独的溶血、肝酶升高和血小板计数降低(HELLP)综合征(p = 0.047)或与产后出血相结合(p = 0.003)、先前接受高渗白蛋白输注治疗(p = 0.001)和氨甲环酸抑制纤溶(p = 0.03)与继发性 ARF 相关。通过多变量分析,唯一的独立因素是 HELLP 综合征与产后出血的联合以及高渗白蛋白输注的使用。
HELLP 综合征伴产后出血会增加复杂产后情况下 ARF 的风险。在这种情况下,应特别注意可能会恶化肾功能的治疗方法。