Haug Jon Birger, Berild Dag, Walberg Mette, Reikvam Åsmund
Department of Infectious Diseases, Oslo University Hospital Trust, Oslo, Norway.
Microbiology Section, Laboratory Centre, Vestre Viken Hospital Trust, Drammen, Norway.
Antimicrob Resist Infect Control. 2014 Dec 24;3(1):40. doi: 10.1186/s13756-014-0040-5. eCollection 2014.
Surveillance data of antibiotic use are increasingly being used for benchmarking purposes, but there is a lack of studies dealing with how hospital- and patient-related factors affect antibiotic utilization in hospitals. Our objective was to identify factors that may contribute to differences in antibiotic use.
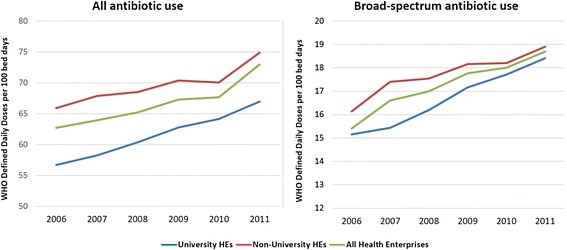
Based on pharmacy sales data (2006-2011), use of all antibiotics, all penicillins, and broad-spectrum antibiotics was analysed in 22 Health Enterprises (HEs). Antibiotic utilization was measured in World Health Organisation defined daily doses (DDDs) and hospital-adjusted (ha)DDDs, each related to the number of bed days (BDs) and the number of discharges. For each HE, all clinical specialties were included and the aggregated data at the HE level constituted the basis for the analyses. Fourteen variables potentially associated with the observed antibiotic use - extracted from validated national databases - were examined in 12 multiple linear regression models, with four different measurement units: DDD/100 BDs, DDD/100 discharges, haDDD/100 BDs and haDDD/100 discharges.
Six variables were independently associated with antibiotic use, but with a variable pattern depending on the regression model. High levels of nurse staffing, high proportions of short (<2 days) and long (>10 days) hospital stays, infectious diseases being the main ICD-10 diagnostic codes, and surgical diagnosis-related groups were correlated with a high use of all antibiotics. University affiliated HEs had a lower level of antibiotic utilization than other institutions in eight of the 12 models, and carried a high explanatory strength. The use of broad-spectrum antibiotics correlated strongly with short and long hospital stays. There was a residual variance (30%-50% for all antibiotics; 60%-70% for broad-spectrum antibiotics) that our analysis did not explain.
The factors associated with hospital antibiotic use were mostly non-modifiable. By adjusting for these factors, it will be easier to evaluate and understand observed differences in antibiotic use between hospitals. Consequently, the inter-hospital differences can be more confidently acted upon. The residual variation is presumed to largely reflect prescriber-related factors.
抗生素使用监测数据越来越多地用于基准测试目的,但缺乏关于医院和患者相关因素如何影响医院抗生素使用情况的研究。我们的目标是确定可能导致抗生素使用差异的因素。
基于药房销售数据(2006 - 2011年),对22家卫生企业(HEs)中所有抗生素、所有青霉素类抗生素和广谱抗生素的使用情况进行了分析。抗生素使用量以世界卫生组织定义的每日剂量(DDDs)和医院调整后的(ha)DDDs来衡量,分别与住院天数(BDs)和出院人数相关。对于每家HE,纳入了所有临床专科,HE层面的汇总数据构成了分析的基础。从经过验证的国家数据库中提取了14个可能与观察到的抗生素使用相关的变量,在12个多元线性回归模型中进行检验,采用四种不同的测量单位:DDD/100个住院日、DDD/100次出院、haDDD/100个住院日和haDDD/100次出院。
六个变量与抗生素使用独立相关,但根据回归模型呈现出不同的模式。护士配备水平高、短住院时间(<2天)和长住院时间(>10天)的比例高、传染病是主要的ICD - 10诊断编码以及手术诊断相关组与所有抗生素的高使用量相关。在12个模型中的8个模型中,大学附属医院的抗生素使用水平低于其他机构,且具有较高的解释力。广谱抗生素的使用与短住院时间和长住院时间密切相关。存在一个我们的分析未解释的剩余方差(所有抗生素为30% - 50%;广谱抗生素为60% - 70%)。
与医院抗生素使用相关的因素大多不可改变。通过对这些因素进行调整,将更容易评估和理解观察到的医院之间抗生素使用的差异。因此,可以更有信心地应对医院间的差异。剩余变异被认为主要反映了与开处方者相关的因素。