Liu Yihua, Frikha Zied, Maureira Pablo, Levy Bruno, Selton-Suty Christine, Villemot Jean-pierre, Huttin Olivier
Department of cardiovascular surgery and heart transplantation, 1, Allée du Morvan, F-54500, Vandoeuvre-lès-Nancy, France.
Department of cardiology, CHU-Nancy, F-54000, France.
J Cardiothorac Surg. 2015 Jan 21;10:8. doi: 10.1186/s13019-015-0208-y.
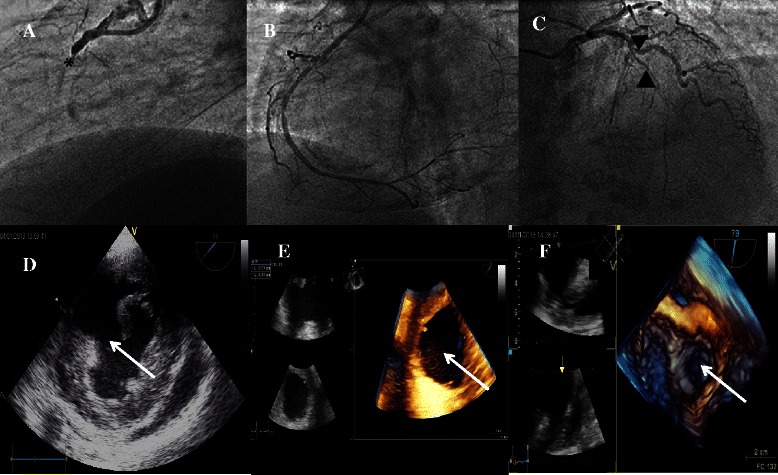
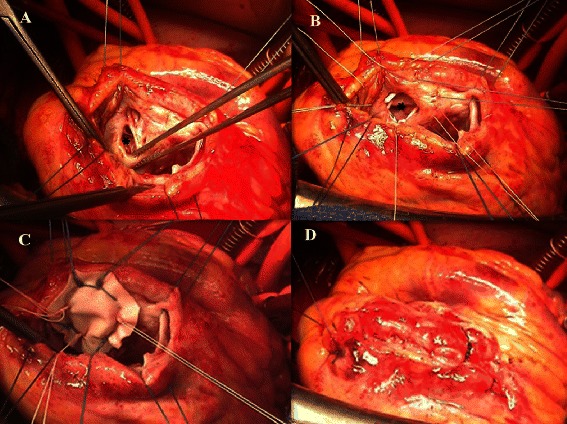
Postinfarction ventricular septal defect (PIVSD) is a devastating mechanical complication following acute myocardial infarction. The management of this pathology is quite challenging, especially in case of complicated cardiogenic shock. The difficulties lie in the timing and type of intervention. Debates exist with regard to immediate versus deferring repair, as well as open repair versus percutaneous closure. The anatomic characteristics and hemodynamic consequence of PIVSD are important elements determining which strategy to adopt, since large septal defect (>15 mm) cannot be appropriately treated by percutaneous occluder devices limiting by their available size, while compromised hemodynamics usually require emergent repair or mechanical support "bridging to surgery". Herein, we report our experience of successful management of a case of cardiogenic shock complicating large PIVSD (38 mm) by delayed surgical repair bridged with Extracorporeal Membrane Oxygenation (ECMO) during 7 days. We emphasize the importance of 3-dimensional transesophageal echocardiography as a decision-making tool.
心肌梗死后室间隔缺损(PIVSD)是急性心肌梗死后一种严重的机械性并发症。这种病症的治疗颇具挑战性,尤其是在并发心源性休克的情况下。困难在于干预的时机和类型。关于立即修复还是延迟修复,以及开放修复还是经皮封堵,存在诸多争议。PIVSD的解剖特征和血流动力学后果是决定采用何种策略的重要因素,因为较大的室间隔缺损(>15毫米)无法通过受可用尺寸限制的经皮封堵装置得到妥善治疗,而血流动力学受损通常需要紧急修复或机械支持“过渡到手术”。在此,我们报告我们成功治疗一例并发大型PIVSD(38毫米)的心源性休克患者的经验,该患者在7天内通过体外膜肺氧合(ECMO)桥接延迟手术修复。我们强调三维经食管超声心动图作为决策工具的重要性。