MGH/MIT/HMS Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA.
Division of Medical Research, Korea Institute of Oriental Medicine, Daejeon, Korea.
Arthritis Rheumatol. 2015 May;67(5):1395-1405. doi: 10.1002/art.39043.
Fibromyalgia (FM) is a chronic functional pain syndrome characterized by widespread pain, significant pain catastrophizing, sympathovagal dysfunction, and amplified temporal summation for evoked pain. While several studies have demonstrated altered resting brain connectivity in FM, studies have not specifically probed the somatosensory system and its role in both somatic and nonsomatic FM symptoms. Our objective was to evaluate resting primary somatosensory cortex (S1) connectivity and to explore how sustained, evoked deep tissue pain modulates this connectivity.
We acquired functional magnetic resonance imaging and electrocardiography data on FM patients and healthy controls during rest (the rest phase) and during sustained mechanical pressure-induced pain over the lower leg (the pain phase). Functional connectivity associated with different S1 subregions was calculated, while S1(leg) connectivity (representation of the leg in the primary somatosensory cortex) was contrasted between the rest phase and the pain phase and was correlated with clinically relevant measures in FM.
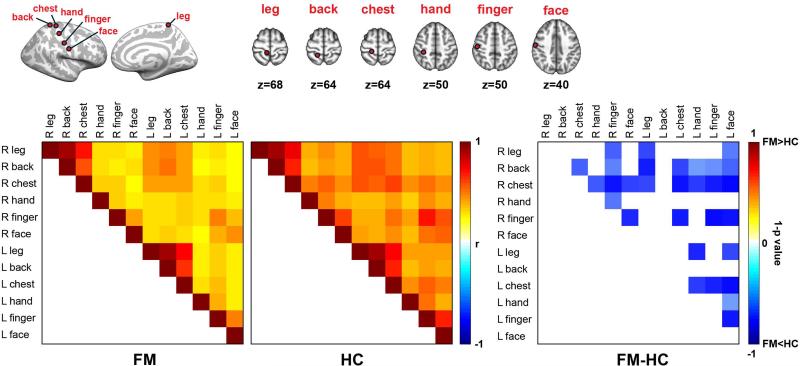
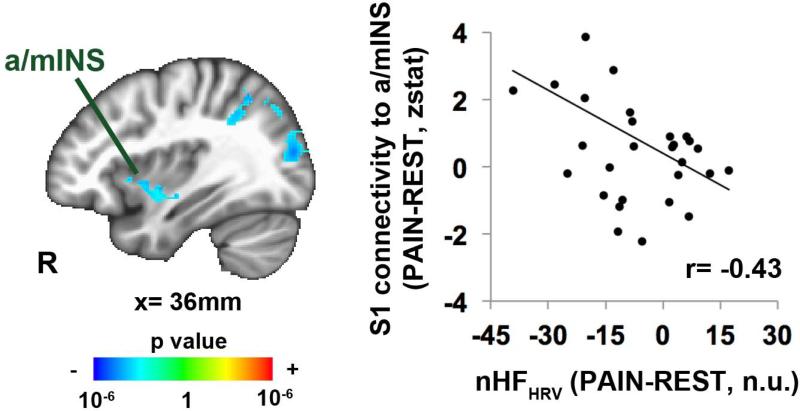
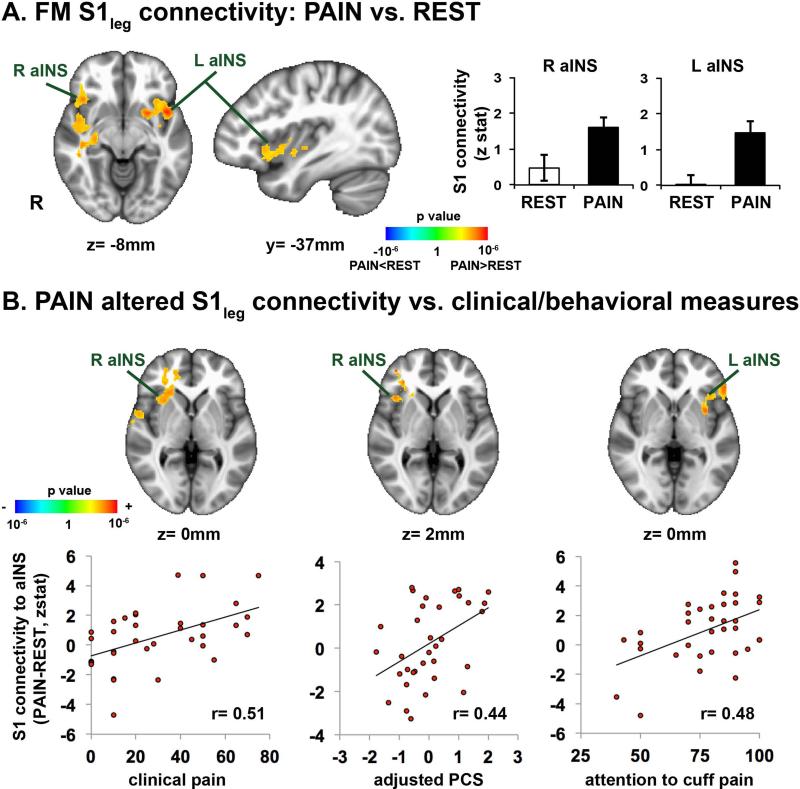
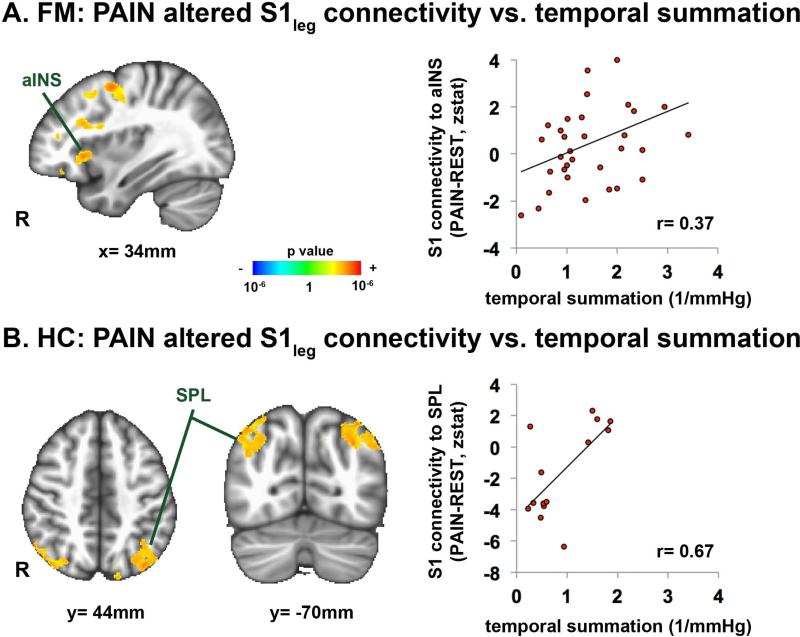
During the rest phase, FM patients showed decreased connectivity between multiple ipsilateral and cross-hemispheric S1 subregions, which was correlated with clinical pain severity. Compared to the rest phase, the pain phase produced increased S1(leg) connectivity to the bilateral anterior insula in FM patients, but not in healthy controls. Moreover, in FM patients, sustained pain-altered S1(leg) connectivity to the anterior insula was correlated with clinical/behavioral pain measures and autonomic responses.
Our study demonstrates that both somatic and nonsomatic dysfunction in FM, including clinical pain, pain catastrophizing, autonomic dysfunction, and amplified temporal summation, are closely linked with the degree to which evoked deep tissue pain alters S1 connectivity to salience/affective pain-processing regions. Additionally, diminished connectivity between S1 subregions during the rest phase in FM may result from ongoing widespread clinical pain.
纤维肌痛(FM)是一种慢性功能性疼痛综合征,其特征为广泛疼痛、显著的疼痛灾难化、交感迷走神经功能障碍以及诱发疼痛的时间总和增强。虽然有几项研究表明 FM 患者静息大脑连接发生改变,但这些研究并未专门探讨躯体感觉系统及其在躯体和非躯体 FM 症状中的作用。我们的目的是评估静息初级躯体感觉皮层(S1)的连接,并探讨持续的、诱发的深部组织疼痛如何调节这种连接。
我们在 FM 患者和健康对照组的静息期(静息期)和小腿持续机械压力诱发疼痛期(疼痛期)采集功能磁共振成像和心电图数据。计算了与不同 S1 亚区相关的功能连接,同时比较了静息期和疼痛期 S1(腿部)的连接(腿部在初级躯体感觉皮层中的代表),并与 FM 中的临床相关指标进行了相关性分析。
在静息期,FM 患者的多个同侧和对侧 S1 亚区之间的连接减少,这与临床疼痛严重程度相关。与静息期相比,疼痛期 FM 患者双侧前岛叶的 S1(腿部)连接增加,但健康对照组无此现象。此外,在 FM 患者中,持续疼痛改变的 S1(腿部)连接前岛叶与临床/行为疼痛指标和自主反应相关。
我们的研究表明,FM 中的躯体和非躯体功能障碍,包括临床疼痛、疼痛灾难化、自主神经功能障碍和时间总和增强,与诱发深部组织疼痛改变 S1 连接到突显/情感疼痛处理区域的程度密切相关。此外,FM 患者在静息期 S1 亚区之间的连接减少可能是由于持续的广泛临床疼痛所致。