David Geffen School of Medicine at University of California, Los Angeles, Division of General Internal Medicine and Health Services Research, UCLA Medicine/GIM, 911 Broxton Avenue, 1st floor, Los Angeles, CA, 90024, USA
Center for Biostatistics, Ohio State University, 2012 Kenny Road, Columbus, Ohio, USA.
BMJ. 2015 Jan 27;350:h25. doi: 10.1136/bmj.h25.
To determine associations between postmenopausal change in body weight and incidence of fracture and associations between voluntary and involuntary weight loss and risk of fracture.
Post hoc analysis of data from the Women's Health Initiative Observational Study and Clinical Trials.
40 clinical centers in the United States.
120,566 postmenopausal women, aged 50-79 at baseline (1993-98), followed through 2013 (mean fracture follow-up duration 11 years from baseline).
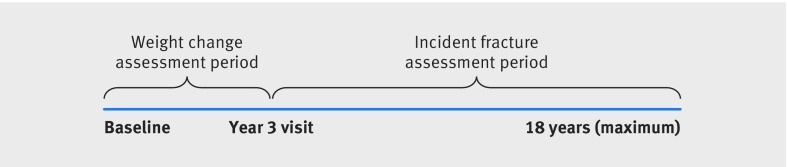
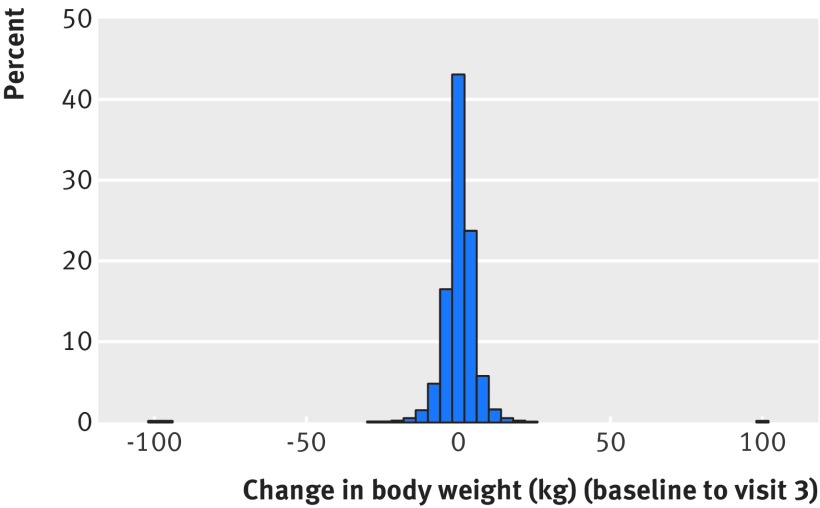
Annualized percentage change in measured body weight from baseline to year 3, classified as stable (<5% change), weight loss (≥ 5%), or weight gain (≥ 5%). Self assessment of whether weight loss was intentional or unintentional. Cox proportional hazards regression models were adjusted for age, race/ethnicity, baseline body mass index (BMI), smoking, alcohol intake, level of physical activity, energy expenditure, calcium and vitamin D intake, physical function score, oophorectomy, hysterectomy, previous fracture, comorbidity score, and drug use.
Incident self reported fractures of the upper limbs, lower limbs, and central body; hip fractures confirmed by medical records.
Mean participant age was 63.3. Mean annualized percent weight change was 0.30% (95% confidence interval 0.28 to 0.32). Overall, 79,279 (65.6%) had stable weight; 18,266 (15.2%) lost weight; and 23,021 (19.0%) gained weight. Compared with stable weight, weight loss was associated with a 65% higher incidence rates of fracture in hip (adjusted hazard ratio 1.65, 95% confidence interval 1.49 to 1.82), upper limb (1.09, 1.03 to 1.16), and central body (1.30, 1.20 to 1.39); weight gain was associated with higher incidence rates of fracture in upper limb (1.10, 1.05 to 1.18) and lower limb (1.18, 1.12 to 1.25). Compared with stable weight, unintentional weight loss was associated with a 33% higher incidence rates of hip fracture (1.33, 1.19 to 1.47) and increased incidence rates of vertebral fracture (1.16, 1.06 to 1.26); intentional weight loss was associated with increased incidence rates of lower limb fracture (1.11, 1.05 to 1.17) and decreased incidence of hip fracture (0.85, 0.76 to 0.95).
Weight gain, weight loss, and intentional weight loss are associated with increased incidence of fracture, but associations differ by fracture location. Clinicians should be aware of fracture patterns after weight gain and weight loss.
确定绝经后体重变化与骨折发生率之间的关联,以及自愿性和非自愿性体重减轻与骨折风险之间的关联。
来自妇女健康倡议观察研究和临床试验的事后分析。
美国 40 个临床中心。
120566 名绝经后女性,基线时年龄为 50-79 岁(1993-98 年),随访至 2013 年(平均骨折随访时间为基线后 11 年)。
从基线到第 3 年测量体重的年化百分比变化,分为稳定(<5%变化)、体重减轻(≥5%)或体重增加(≥5%)。自我评估体重减轻是有意还是无意的。Cox 比例风险回归模型调整了年龄、种族/民族、基线体重指数(BMI)、吸烟、饮酒量、身体活动水平、能量消耗、钙和维生素 D 摄入量、身体功能评分、卵巢切除术、子宫切除术、既往骨折、合并症评分和药物使用。
上肢、下肢和中央体的自我报告骨折;经病历证实的髋部骨折。
平均参与者年龄为 63.3 岁。平均年化体重变化百分比为 0.30%(95%置信区间 0.28 至 0.32)。总体而言,79279 人(65.6%)体重稳定;18266 人(15.2%)体重减轻;23021 人(19.0%)体重增加。与体重稳定相比,体重减轻与髋部(调整后的危险比 1.65,95%置信区间 1.49 至 1.82)、上肢(1.09,1.03 至 1.16)和中央体(1.30,1.20 至 1.39)骨折发生率增加 65%相关;体重增加与上肢(1.10,1.05 至 1.18)和下肢(1.18,1.12 至 1.25)骨折发生率增加相关。与体重稳定相比,非自愿性体重减轻与髋部骨折发生率增加 33%(1.33,1.19 至 1.47)和椎体骨折发生率增加(1.16,1.06 至 1.26)相关;有意的体重减轻与下肢骨折发生率增加(1.11,1.05 至 1.17)和髋部骨折发生率降低(0.85,0.76 至 0.95)相关。
体重增加、体重减轻和有意的体重减轻与骨折发生率增加有关,但关联因骨折部位而异。临床医生应注意体重增加和体重减轻后的骨折模式。