Chen Xin-Zu, Wen Lei, Rui Yuan-Yi, Liu Chao-Xu, Zhao Qing-Chuan, Zhou Zong-Guang, Hu Jian-Kun
From the Department of Gastrointestinal Surgery, West China Hospital, Sichuan University, China (XZC, YYR, ZGZ, JKH); Department of Surgery, Xijing Hospital of Digestive Diseases, The Fourth Military Medical University, China (LW, CXL, QCZ).
Medicine (Baltimore). 2015 Jan;94(4):e454. doi: 10.1097/MD.0000000000000454.
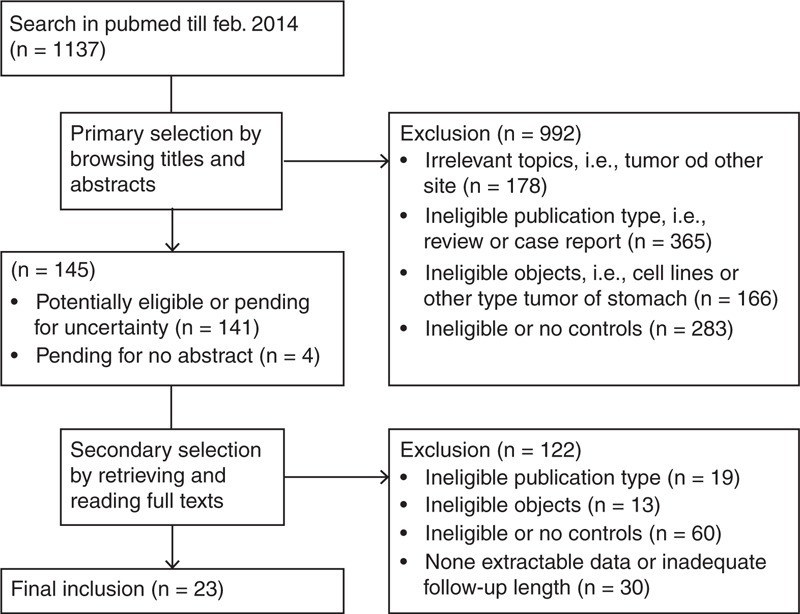
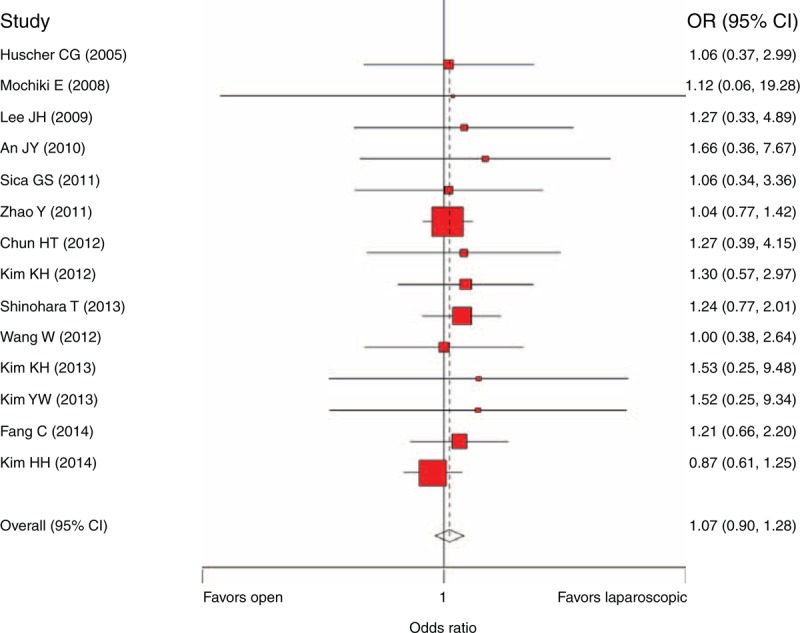
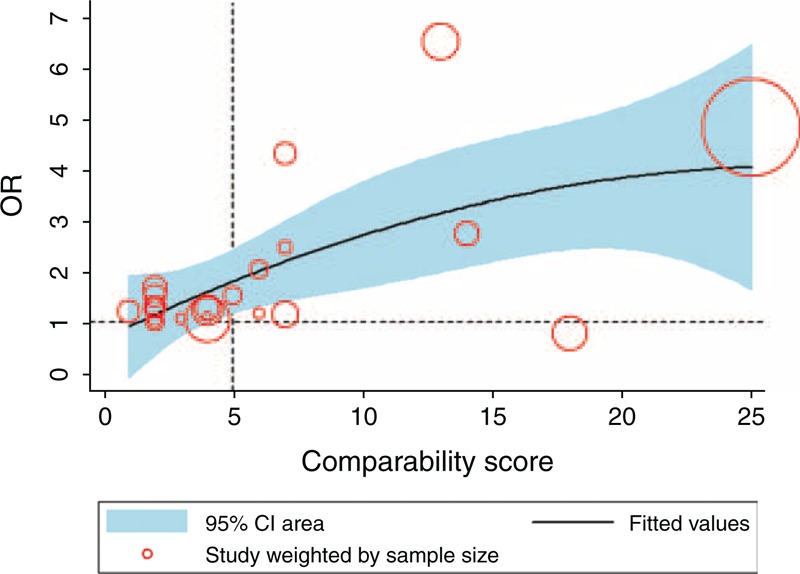
Many meta-analyses have confirmed the technical feasibility and favorable short-term surgical outcomes of laparoscopic gastrectomy (LG) for gastric cancer patients, but the long-term survival outcome of LG remains controversial compared with open gastrectomy (OG). This study aimed to compare the 5-year overall survival (OS), recurrence, and gastric cancer-related death of LG with OG among gastric cancer patients. PubMed was searched to February 2014. The resectable gastric cancer patients who underwent curative LG or OG were eligible. The studies that compared 5-year OS, recurrence, or gastric cancer-related death in the LG and OG groups were included. A meta-analysis, meta-regression, sensitivity analysis, subgroup analysis, and stage-specific analysis were performed to estimate the survival outcome between the two groups and identify the potential confounders. Quality assessment was based on a tailored comparability scoring system. Twenty-three studies with 7336 patients were included. The score of comparability between two groups and the extent of lymphadenectomy were two independent confounders. Based on the well-balanced studies, the 5-year OS (OR = 1.07, 95% CI 0.90-1.28, P = 0.45), recurrence (OR = 0.83, 95% CI 0.68-1.02, P = 0.08), and gastric cancer-related death (OR = 0.86, 95% CI 0.65-1.13, P = 0.28) rates were comparable in LG and OG. Several subsets such as the publication year, study region, sample size, gastrectomy pattern, extent of lymphadenectomy, number of nodes harvested, and proportion of T1-2 or N0-1 did not influence the estimates, if they were well balanced. Particularly, the stage-specific estimates obtained comparable results between the two groups. Randomized controlled trials comparing LG with OG remain sparse to assess their long-term survival outcomes. The major contributions of this systematic review compared with other meta-analyses are a comprehensive collection of available long-term survival outcomes within a much larger number of observations and a more precise consideration of confounders. Current knowledge indicates that the long-term survival outcome of laparoscopic gastric cancer surgery is comparable to that of open surgery among early or advanced stage gastric cancer patients, and LG is acceptable with regard to oncologic safety.
许多荟萃分析已经证实了腹腔镜胃癌切除术(LG)对胃癌患者的技术可行性和良好的短期手术效果,但与开放胃癌切除术(OG)相比,LG的长期生存结果仍存在争议。本研究旨在比较LG与OG在胃癌患者中的5年总生存率(OS)、复发率和胃癌相关死亡率。检索了截至2014年2月的PubMed。接受根治性LG或OG的可切除胃癌患者符合条件。纳入比较LG组和OG组5年OS、复发率或胃癌相关死亡率的研究。进行了荟萃分析、荟萃回归、敏感性分析、亚组分析和分期特异性分析,以评估两组之间的生存结果并确定潜在的混杂因素。质量评估基于定制的可比性评分系统。纳入了23项研究,共7336例患者。两组之间的可比性得分和淋巴结清扫范围是两个独立的混杂因素。基于均衡的研究,LG和OG的5年OS(OR = 1.07,95% CI 0.90 - 1.28,P = 0.45)、复发率(OR = 0.83,95% CI 0.68 - 1.02,P = 0.08)和胃癌相关死亡率(OR = 0.86,95% CI 0.65 - 1.13,P = 0.28)相当。如果几个子集(如发表年份、研究地区、样本量、胃切除术模式、淋巴结清扫范围、获取的淋巴结数量以及T1 - 2或N0 - 1的比例)是均衡的,则不会影响估计值。特别是,分期特异性估计在两组之间获得了可比的结果。比较LG与OG的随机对照试验仍然很少,无法评估它们的长期生存结果。与其他荟萃分析相比,本系统评价的主要贡献在于在大量观察结果中全面收集了可用的长期生存结果,并更精确地考虑了混杂因素。目前的知识表明,在早期或晚期胃癌患者中,腹腔镜胃癌手术的长期生存结果与开放手术相当,并且就肿瘤学安全性而言,LG是可以接受的。