Alfirevic Zarko, Keeney Edna, Dowswell Therese, Welton Nicky J, Dias Sofia, Jones Leanne V, Navaratnam Kate, Caldwell Deborah M
Centre for Women's Health Research, University of Liverpool and Liverpool Women's Hospital, Liverpool L8 7SS, UK
School of Social and Community Medicine, University of Bristol, Bristol BS8 2PS, UK.
BMJ. 2015 Feb 5;350:h217. doi: 10.1136/bmj.h217.
To assess the effectiveness and safety of prostaglandins used for labour induction.
Systematic review with Bayesian network meta-analysis
The Cochrane Pregnancy and Childbirth Group's Database of Trials (which incorporates the results of a broad generic search for all pregnancy and postpartum trials). Sources included are CENTRAL, Medline, Embase, NHS Economic Evaluation Database, CINAHL, relevant journals, conference proceedings, and registries of ongoing trials.
Randomised clinical trials of prostaglandin or prostaglandin analogues used for third trimester cervical ripening or labour induction versus placebo or no treatment, alternative prostaglandin dose or administration, or a different type of prostaglandin. We included studies recruiting women with a viable fetus, but had no other restrictions relating to indication for labour induction or language of publication. Outcomes assessed were serious neonatal morbidity (trialist defined) or perinatal death; serious maternal morbidity (trialist defined) or death; vaginal delivery not achieved within 24 hours, caesarean section, and uterine hyperstimulation with fetal heart rate changes.
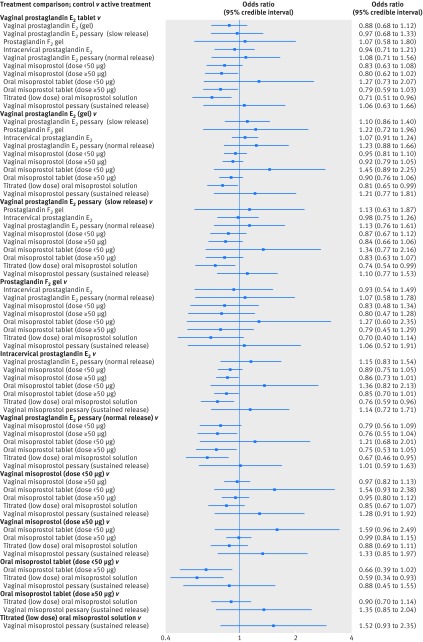
280 randomised clinical trials were included (48 068 women) in the review. Maternal and neonatal mortality and serious morbidity were rarely reported and are summarized narratively. Unresolved inconsistency was observed for the hyperstimulation outcome. Relative to placebo, the odds of failing to achieve a vaginal delivery were lowest for vaginal misoprostol (≥50 µg) (odds ratio 0.06 (95% credible interval 0.02 to 0.12)), with a 39% absolute probability of event (95% credible interval 1% to 94%). Compared with placebo, odds of caesarean section were lowest for titrated oral misoprostol solution (<50 µg) (odds ratio 0.65 (0.49 to 0.83)), with an absolute probability of event of 15% (3% to 40%).
Low dose(<50 µg) titrated oral misoprostol solution had the lowest probability of caesarean section, whereas vaginal misprostol (≥50 µg) had the highest probability of achieving a vaginal delivery within 24 hours. These findings have important implications for a series of current national and international guidelines for induction of labour and future research in this area.
PROSPERO 2013:CRD42013005116.
评估用于引产的前列腺素的有效性和安全性。
采用贝叶斯网络荟萃分析的系统评价
Cochrane妊娠与分娩组试验数据库(其中纳入了对所有妊娠和产后试验进行广泛综合检索的结果)。包括的来源有Cochrane系统评价数据库、医学期刊数据库、荷兰医学文摘数据库、英国国家医疗服务体系经济评估数据库、护理学与健康领域数据库、相关期刊、会议论文集以及正在进行的试验注册库。
前列腺素或前列腺素类似物用于孕晚期宫颈成熟或引产与安慰剂或不治疗、不同前列腺素剂量或给药方式、或不同类型前列腺素的随机临床试验。我们纳入了招募有存活胎儿的女性的研究,但对引产指征或发表语言没有其他限制。评估的结局包括严重新生儿发病率(由试验者定义)或围产期死亡;严重孕产妇发病率(由试验者定义)或死亡;24小时内未实现阴道分娩、剖宫产以及伴有胎儿心率变化的子宫过度刺激。
该评价纳入了280项随机临床试验(48068名女性)。孕产妇和新生儿死亡率及严重发病率很少被报告,以叙述形式进行总结。对于子宫过度刺激结局,观察到未解决的不一致性。相对于安慰剂,阴道用米索前列醇(≥50μg)未能实现阴道分娩的几率最低(比值比0.06(95%可信区间0.02至0.12)),事件的绝对概率为39%(95%可信区间1%至94%)。与安慰剂相比,滴定口服米索前列醇溶液(<50μg)剖宫产的几率最低(比值比0.65(0.49至0.83)),事件的绝对概率为15%(3%至40%)。
低剂量(<50μg)滴定口服米索前列醇溶液剖宫产的概率最低,而阴道用米索前列醇(≥50μg)在24小时内实现阴道分娩的概率最高。这些发现对当前一系列国内和国际引产指南以及该领域的未来研究具有重要意义。
PROSPERO 2013:CRD42013005116。