Riall Taylor S, Adhikari Deepak, Parmar Abhishek D, Linder Suzanne K, Dimou Francesca M, Crowell Winston, Tamirisa Nina P, Townsend Courtney M, Goodwin James S
Department of Surgery, The University of Texas Medical Branch, Galveston, TX.
Department of Surgery, The University of Texas Medical Branch, Galveston, TX.
J Am Coll Surg. 2015 Apr;220(4):682-90. doi: 10.1016/j.jamcollsurg.2014.12.012. Epub 2014 Dec 17.
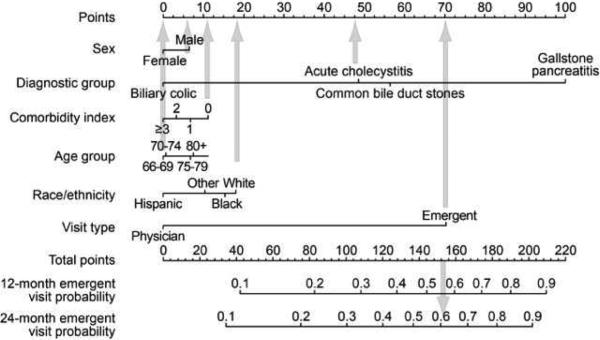
We recently developed and validated a prognostic model that accurately predicts the 2-year risk of emergent gallstone-related hospitalization in older patients presenting with symptomatic gallstones.
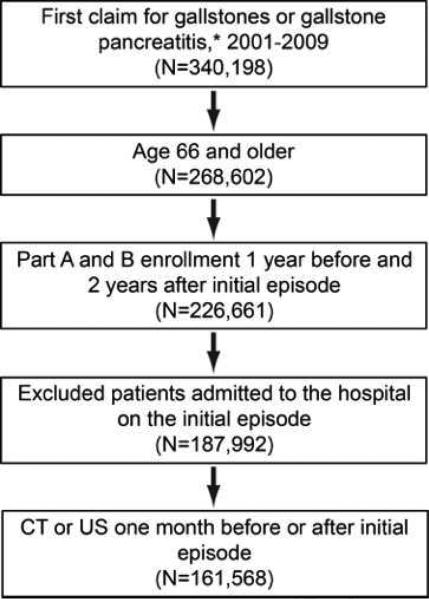
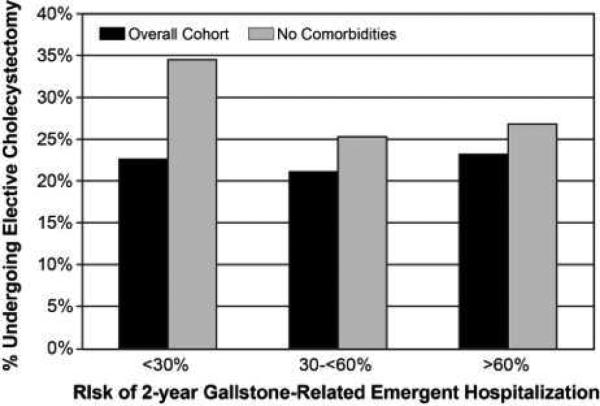
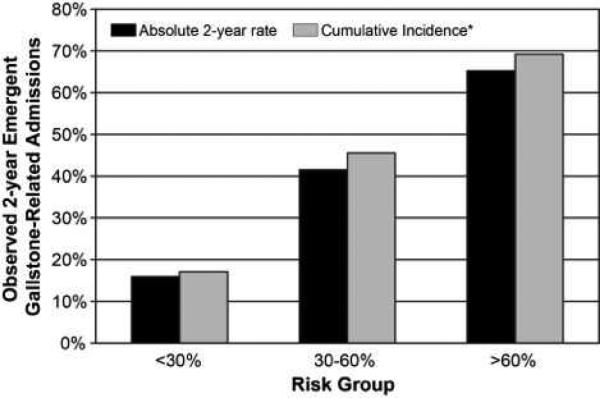
We used 100% Texas Medicare data (2000 to 2011) to identify patients aged 66 years and older with an initial episode of symptomatic gallstones not requiring emergency hospitalization. At presentation, we calculated each patient's risk of 2-year gallstone-related emergent hospitalization using the previously validated model. Patients were placed into the following risk groups based on model estimates: <30%, 30% to <60%, and ≥ 60%. Within each risk group, we calculated the percent of elective cholecystectomies (≤ 2.5 months from initial episode) performed.
In all, 161,568 patients had an episode of symptomatic gallstones. Mean age was 76.5 ± 7.3 years and 59.9% were female. The 2-year risk of gallstone-related hospitalizations increased from 15.9% to 41.5% to 65.2% across risk groups. For the overall cohort, 22.3% in the low-risk group, 20.9% in the moderate-risk group, and 23.2% in the high-risk group underwent elective cholecystectomy in the 2.5 months after the initial symptomatic episode. In patients with no comorbidities, elective cholecystectomy rates decreased from 34.2% in the low-risk group to 26.7% in the high-risk group. Of patients who did not undergo cholecystectomy, only 9.5% were seen by a surgeon in the 2.5 months after the initial episode.
The risk of recurrent acute biliary symptoms requiring hospitalization has no influence, or even a paradoxical negative influence, on the decision to perform elective cholecystectomy after an initial symptomatic episode. Translation of the risk prediction model into clinical practice can better align treatment with risk and improve outcomes in older patients with symptomatic gallstones.
我们最近开发并验证了一种预后模型,该模型可准确预测有症状胆结石的老年患者发生与胆结石相关的紧急住院的2年风险。
我们使用100%的德克萨斯医疗保险数据(2000年至2011年)来识别66岁及以上初次出现有症状胆结石且无需紧急住院治疗的患者。就诊时,我们使用先前验证的模型计算每位患者2年胆结石相关紧急住院的风险。根据模型估计,将患者分为以下风险组:<30%、30%至<60%和≥60%。在每个风险组内,我们计算了(在初次发病后≤2.5个月内)进行择期胆囊切除术的百分比。
共有161,568例患者出现有症状胆结石。平均年龄为76.5±7.3岁,59.9%为女性。跨风险组,与胆结石相关的住院2年风险从15.9%增至41.5%再到65.2%。对于整个队列,低风险组22.3%、中风险组20.9%、高风险组23.2%在初次出现症状后的2.5个月内接受了择期胆囊切除术。在无合并症的患者中,择期胆囊切除术率从低风险组的34.2%降至高风险组的26.7%。在未接受胆囊切除术的患者中,初次发病后2.5个月内只有9.5%的患者看过外科医生。
需要住院治疗的复发性急性胆道症状的风险对初次出现症状后进行择期胆囊切除术的决策没有影响,甚至有反常的负面影响。将风险预测模型转化为临床实践可以使治疗更好地与风险相匹配,并改善有症状胆结石老年患者的治疗效果。