Suidan Rudy S, Zhou Qin, Iasonos Alexia, O'Cearbhaill Roisin E, Chi Dennis S, Long Roche Kara C, Tanner Edward J, Denesopolis John, Barakat Richard R, Zivanovic Oliver
*Gynecology Service, Department of Surgery, †Department of Epidemiology and Biostatistics, and ‡Gynecologic Medical Oncology Service, Department of Medicine, Memorial Sloan Kettering Cancer Center; and §Weill Cornell Medical College, New York, NY.
Int J Gynecol Cancer. 2015 May;25(4):599-606. doi: 10.1097/IGC.0000000000000389.
Phase 3 trials have demonstrated a survival advantage for patients with optimally debulked epithelial ovarian cancer who received intravenous (IV) and intraperitoneal (IP) chemotherapy compared with IV therapy alone. This was despite a significant proportion of patients in the IV/IP arms not completing all 6 planned cycles. Our objective was to evaluate the prognostic significance of the number of IV/IP cycles administered.
METHODS/MATERIALS: Data were analyzed for all patients with stage III to IV epithelial ovarian cancer who underwent optimal primary cytoreduction followed by 1 or more cycles of IV/IP chemotherapy from January 2005 to July 2011 at our institution. A landmark analysis was performed to associate progression-free survival (PFS) and overall survival (OS) with the number of IV/IP cycles given.
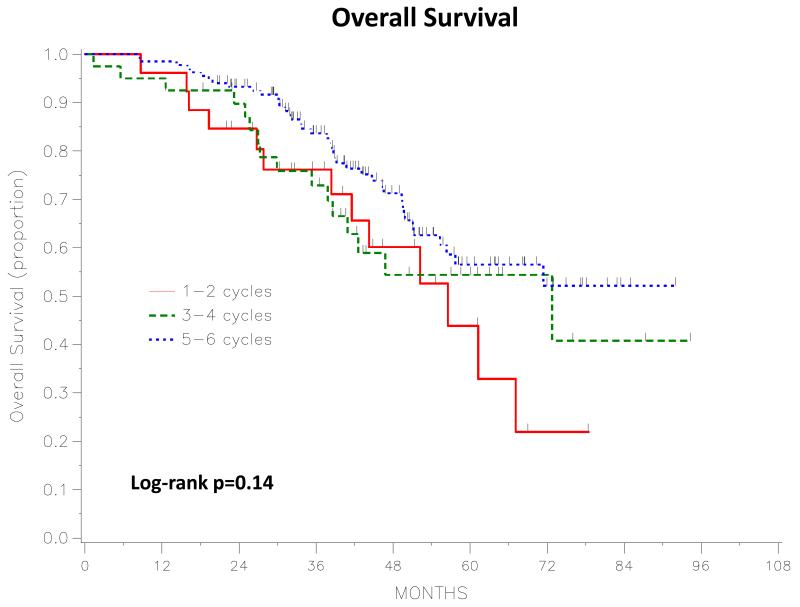
We identified 201 patients; 26 (13%) received 1 to 2 cycles of IV/IP chemotherapy, 41 (20%) received 3 to 4 cycles, and 134 (67%) received 5 to 6 cycles. The 5-year PFS for patients who received 1 to 2, 3 to 4, and 5 to 6 cycles was 18%, 29%, and 17%, respectively. The 5-year OS for patients who received 1 to 2, 3 to 4, and 5 to 6 cycles was 44%, 54%, and 57%, respectively. There was no significant difference in PFS (P = 0.31) or OS (P = 0.14) between the 3 groups. The most common reason for discontinuing IV/IP therapy was treatment-related toxicity (77%). Postoperative complications were the most common reason for not initiating IV/IP therapy (42%) in patients who subsequently transitioned to it.
We did not detect a significant survival difference between patients who received 1 to 2, 3 to 4, or 5 to 6 IV/IP chemotherapy cycles. Women may still derive a survival benefit if they receive fewer than 6 IV/IP cycles.
3期试验已证明,与单纯静脉化疗相比,接受静脉(IV)和腹腔内(IP)化疗的上皮性卵巢癌患者若达到最佳肿瘤细胞减灭术则具有生存优势。尽管接受IV/IP联合化疗的患者中有很大一部分未完成全部6个计划周期的治疗。我们的目的是评估给予IV/IP化疗周期数的预后意义。
方法/材料:分析了2005年1月至2011年7月在我院接受最佳初次细胞减灭术并随后进行1个或更多周期IV/IP化疗的所有III至IV期上皮性卵巢癌患者的数据。进行了一项里程碑分析,以将无进展生存期(PFS)和总生存期(OS)与给予的IV/IP化疗周期数相关联。
我们纳入了201例患者;26例(13%)接受了1至2个周期的IV/IP化疗,41例(20%)接受了3至4个周期,134例(67%)接受了5至6个周期。接受1至2个、3至4个以及5至6个周期化疗的患者的5年PFS分别为18%、29%和17%。接受1至2个、3至4个以及5至6个周期化疗的患者的5年OS分别为44%、54%和57%。三组之间的PFS(P = 0.31)或OS(P = 0.14)无显著差异。停止IV/IP治疗的最常见原因是治疗相关毒性(77%)。术后并发症是随后转为接受IV/IP治疗的患者中未开始该治疗的最常见原因(42%)。
我们未检测到接受1至2个、3至4个或5至6个IV/IP化疗周期的患者之间存在显著的生存差异。女性若接受少于6个IV/IP周期的化疗仍可能获得生存益处。