Chevinsky Michael, Imnadze Mariam, Sankin Alexander, Winer Andrew, Mano Roy, Jakubowski Christopher, Mashni Joseph, Sjoberg Daniel D, Chen Ying-Bei, Tickoo Satish K, Reuter Victor E, Hakimi A Ari, Russo Paul
Urology Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, New York.
J Urol. 2015 Aug;194(2):310-5. doi: 10.1016/j.juro.2015.02.013. Epub 2015 Feb 9.
Tumor size and stage are important prognostic parameters in renal cell carcinoma. While pathological stage T1 and T2 are defined by size alone, the presence of certain intrinsic features can up stage a tumor to pathological stage T3a regardless of size. We investigate the effect of pathological tumor stage on the relationship between tumor size and risk of disease recurrence.
Data were reviewed on patients who underwent nephrectomy at our institution between 2006 and 2013 to identify all those with pathological stage T1, T2 and T3a tumors. A proportional hazards Cox model was built with time to recurrence as outcome, and pathological stage and tumor size as covariates. An interaction term for stage and tumor size was included.
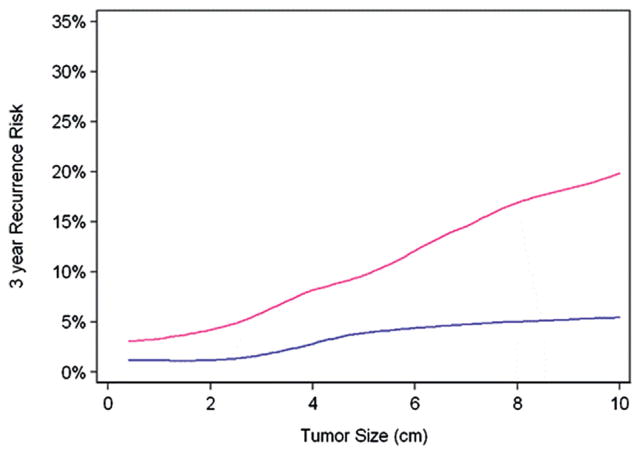
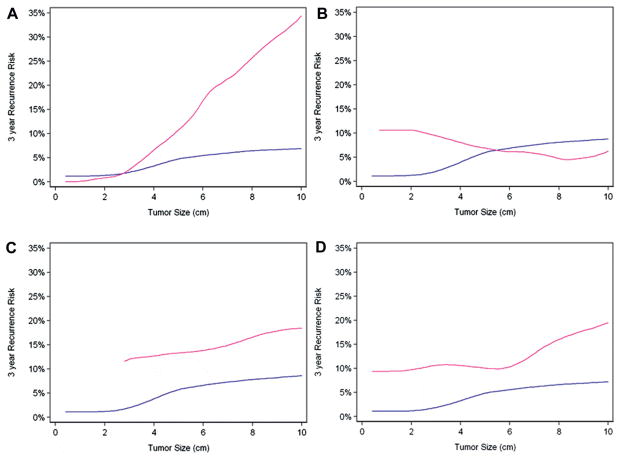
The final cohort included 1,809 patients. On multivariable analysis, when adjusted for tumor size, patients with pT3a tumors had a greater risk of tumor recurrence compared to those with pT1/T2 tumors (HR 3.70; 95% CI 2.31, 5.92; p <0.0001). The risk of disease recurrence increased more rapidly as tumor size increased only with the presence of perinephric fat invasion (p=0.006).
Using the AJCC 2010 staging criteria we validated pathological stage T3a as a poor prognostic factor in renal cell carcinoma regardless of tumor size. Our results also demonstrated an increased rate of risk of recurrence with perinephric fat invasion. Given this increased risk of recurrence, even in tumors less than 4 cm, closer surveillance is warranted in such cases and the role of perinephric involvement necessitates further investigation.
肿瘤大小和分期是肾细胞癌重要的预后参数。虽然病理分期T1和T2仅由大小定义,但某些内在特征的存在可使肿瘤不论大小均上调至病理分期T3a。我们研究了病理肿瘤分期对肿瘤大小与疾病复发风险之间关系的影响。
回顾了2006年至2013年在本机构接受肾切除术患者的数据,以确定所有病理分期为T1、T2和T3a肿瘤的患者。构建了一个以复发时间为结局、病理分期和肿瘤大小为协变量的比例风险Cox模型。纳入了分期与肿瘤大小的交互项。
最终队列包括1809例患者。多变量分析显示,在调整肿瘤大小后,pT3a肿瘤患者与pT1/T2肿瘤患者相比,肿瘤复发风险更高(风险比3.70;95%置信区间2.31,5.92;p<0.0001)。仅在存在肾周脂肪浸润时,疾病复发风险随肿瘤大小增加而增加得更快(p=0.006)。
使用美国癌症联合委员会(AJCC)2010年分期标准,我们验证了病理分期T3a是肾细胞癌的一个不良预后因素,不论肿瘤大小如何。我们的结果还表明,肾周脂肪浸润会增加复发风险。鉴于这种复发风险增加,即使在肿瘤小于4 cm的情况下,此类病例也需要更密切的监测,肾周受累的作用需要进一步研究。