Li Ying, Rodrigues Anna, Li Taoran, Yuan Lulin, Yin Fang-Fang, Wu Q Jackie
Department of Oncology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, 400016, China.
J Appl Clin Med Phys. 2015 Jan 8;16(1):5137. doi: 10.1120/jacmp.v16i1.5137.
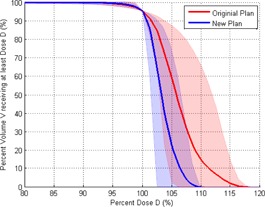
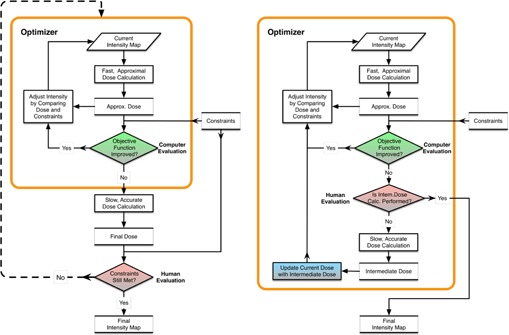
The purpose of this study was to evaluate the effect of dose calculation accuracy and the use of an intermediate dose calculation step during the optimization of intensity-modulated radiation therapy (IMRT) planning on the final plan quality for lung cancer patients. This study included replanning for 11 randomly selected free-breathing lung IMRT plans. The original plans were optimized using a fast pencil beam convolution algorithm. After optimization, the final dose calculation was performed using the analytical anisotropic algorithm (AAA). The Varian Treatment Planning System (TPS) Eclipse v11, includes an option to perform intermediate dose calculation during optimization using the AAA. The new plans were created using this intermediate dose calculation during optimization with the same planning objectives and dose constraints as in the original plan. Differences in dosimetric parameters for the planning target volume (PTV) dose coverage, organs-at-risk (OARs) dose sparing, and the number of monitor units (MU) between the original and new plans were analyzed. Statistical significance was determined with a p-value of less than 0.05. All plans were normalized to cover 95% of the PTV with the prescription dose. Compared with the original plans, the PTV in the new plans had on average a lower maximum dose (69.45 vs. 71.96Gy, p = 0.005), a better homogeneity index (HI) (0.08 vs. 0.12, p = 0.002), and a better conformity index (CI) (0.69 vs. 0.59, p = 0.003). In the new plans, lung sparing was increased as the volumes receiving 5, 10, and 30 Gy were reduced when compared to the original plans (40.39% vs. 42.73%, p = 0.005; 28.93% vs. 30.40%, p = 0.001; 14.11%vs. 14.84%, p = 0.031). The volume receiving 20 Gy was not significantly lower (19.60% vs. 20.38%, p = 0.052). Further, the mean dose to the lung was reduced in the new plans (11.55 vs. 12.12 Gy, p = 0.024). For the esophagus, the mean dose, the maximum dose, and the volumes receiving 20 and 60 Gy were lower in the new plans than in the original plans (17.91 vs. 19.24 Gy, p = 0.004; 57.32vs. 59.81 Gy, p = 0.020; 39.34% vs. 41.59%, p = 0.097; 12.56%vs. 15.35%, p = 0.101). For the heart, the mean dose, the maximum dose, and the volume receiving 40 Gy were also lower in new plans (11.07 vs. 12.04 Gy, p = 0.007; 56.41 vs. 57.7 Gy, p = 0.027; 7.16% vs. 9.37%, p= 0.012). The maximum dose to the spinal cord in the new plans was significantly lower than in the original IMRT plans (29.1 vs. 31.39Gy, p = 0.014). Difference in MU between the IMRT plans was not significant (1216.90 vs. 1198.91, p = 0.328). In comparison to the original plans, the number of iterations needed to meet the optimization objectives in the new plans was reduced by a factor of 2 (2-3 vs. 5-6 iterations). Further, optimization was 30% faster corresponding to an average time savings of 10-15 min for the reoptimized plans. Accuracy of the dose calculation algorithm during optimization has an impact on planning efficiency, as well as on the final plan dosimetric quality. For lung IMRT treatment planning, utilizing the intermediate dose calculation during optimization is feasible for dose homogeneity improvement of the PTV and for improvement of optimization efficiency.
本研究的目的是评估在肺癌患者调强放射治疗(IMRT)计划优化过程中剂量计算准确性以及使用中间剂量计算步骤对最终计划质量的影响。本研究包括对11个随机选择的自由呼吸肺部IMRT计划进行重新规划。原始计划使用快速铅笔束卷积算法进行优化。优化后,使用分析各向异性算法(AAA)进行最终剂量计算。瓦里安治疗计划系统(TPS)Eclipse v11包括一个选项,可在优化过程中使用AAA进行中间剂量计算。新计划是在优化过程中使用此中间剂量计算创建的,其规划目标和剂量约束与原始计划相同。分析了原始计划和新计划之间在计划靶区(PTV)剂量覆盖、危及器官(OARs)剂量 sparing以及监测单位(MU)数量等剂量学参数方面的差异。以p值小于0.05确定统计学显著性。所有计划均进行归一化处理,以使PTV的95%覆盖处方剂量。与原始计划相比,新计划中的PTV平均最大剂量较低(69.45对71.96Gy,p = 0.005),均匀性指数(HI)更好(0.08对0.12,p = 0.002),适形指数(CI)更好(0.69对0.59,p = 0.003)。在新计划中,与原始计划相比,接受5、10和30 Gy的肺体积减少,肺 sparing增加(40.39%对42.73%,p = 0.005;28.93%对30.40%,p = 0.001;14.11%对14.84%,p = 0.031)。接受20 Gy的体积没有显著降低(19.60%对20.38%,p = 0.052)。此外,新计划中肺平均剂量降低(11.55对12.12 Gy,p = 0.024)。对于食管,新计划中的平均剂量、最大剂量以及接受20和60 Gy的体积均低于原始计划(17.91对19.24 Gy,p = 0.004;57.32对59.81 Gy,p = 0.020;39.34%对41.59%,p = 0.097;12.56%对15.35%,p = 0.101)。对于心脏,新计划中的平均剂量、最大剂量以及接受40 Gy的体积也较低(11.07对12.04 Gy,p = 0.007;56.41对57.7 Gy,p = 0.027;7.16%对9.37%,p = 0.012)。新计划中脊髓的最大剂量显著低于原始IMRT计划(29.1对31.39Gy,p = 0.014)。IMRT计划之间的MU差异不显著(1216.90对1198.91,p = 0.328)。与原始计划相比,新计划中达到优化目标所需的迭代次数减少了一半(2 - 3次对5 - 6次迭代)。此外,优化速度提高了30%,重新优化后的计划平均节省时间10 - 15分钟。优化过程中剂量计算算法的准确性对计划效率以及最终计划剂量学质量都有影响。对于肺部IMRT治疗计划,在优化过程中利用中间剂量计算对于改善PTV的剂量均匀性和提高优化效率是可行的。