Hammer Niels, Glätzner Juliane, Feja Christine, Kühne Christian, Meixensberger Jürgen, Planitzer Uwe, Schleifenbaum Stefan, Tillmann Bernhard N, Winkler Dirk
Institute of Anatomy, University of Leipzig, Faculty of Medicine, Leipzig, Germany.
Department of Neurosurgery, University Clinic of Leipzig, Faculty of Medicine, Leipzig, Germany.
PLoS One. 2015 Feb 13;10(2):e0118006. doi: 10.1371/journal.pone.0118006. eCollection 2015.
Vagus nerve stimulation is increasingly applied to treat epilepsy, psychiatric conditions and potentially chronic heart failure. After implanting vagus nerve electrodes to the cervical vagus nerve, side effects such as voice alterations and dyspnea or missing therapeutic effects are observed at different frequencies. Cervical vagus nerve branching might partly be responsible for these effects. However, vagus nerve branching has not yet been described in the context of vagus nerve stimulation.
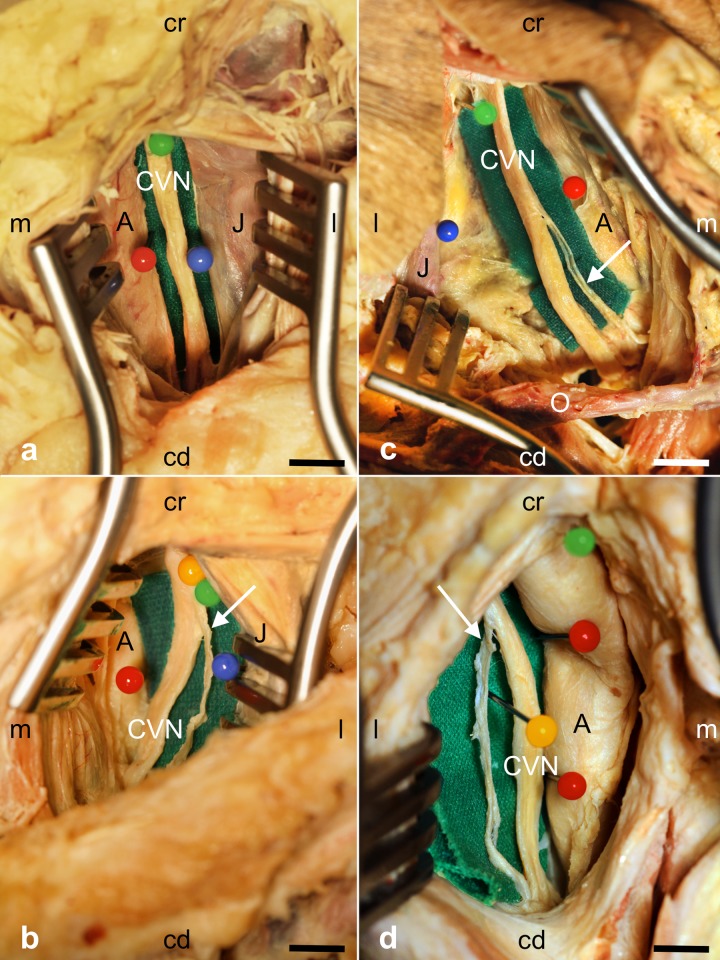
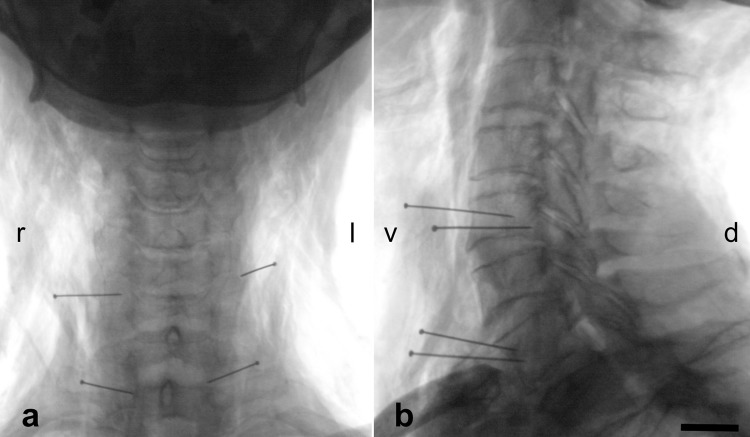
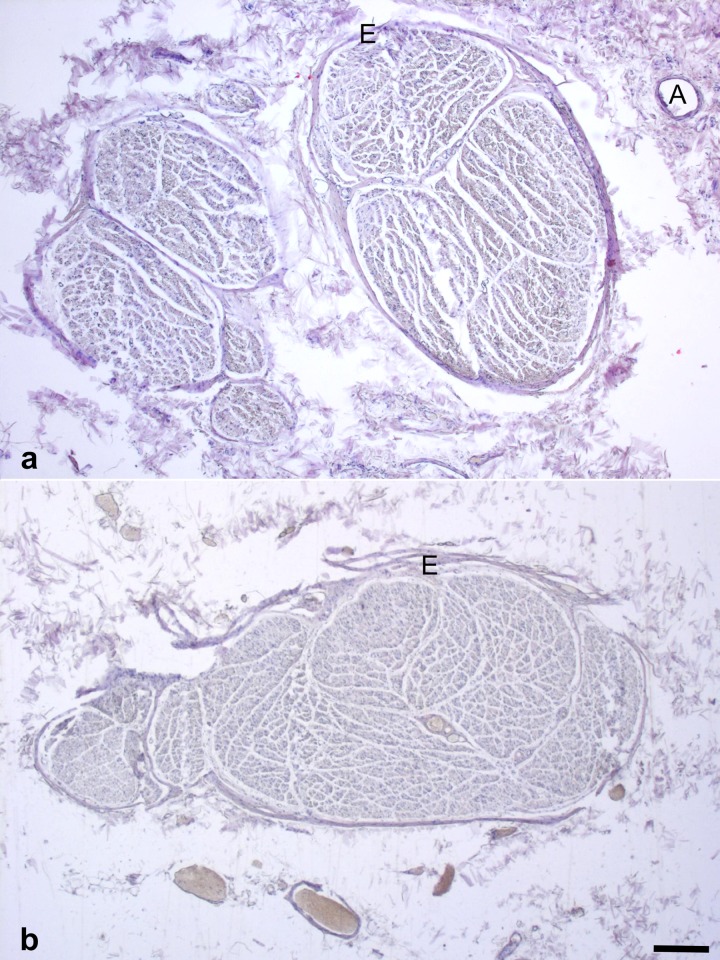
Branching of the cervical vagus nerve was investigated macroscopically in 35 body donors (66 cervical sides) in the carotid sheath. After X-ray imaging for determining the vertebral levels of cervical vagus nerve branching, samples were removed to confirm histologically the nerve and to calculate cervical vagus nerve diameters and cross-sections.
Cervical vagus nerve branching was observed in 29% of all cases (26% unilaterally, 3% bilaterally) and proven histologically in all cases. Right-sided branching (22%) was more common than left-sided branching (12%) and occurred on the level of the fourth and fifth vertebra on the left and on the level of the second to fifth vertebra on the right side. Vagus nerves without branching were significantly larger than vagus nerves with branches, concerning their diameters (4.79 mm vs. 3.78 mm) and cross-sections (7.24 mm2 vs. 5.28 mm2).
Cervical vagus nerve branching is considerably more frequent than described previously. The side-dependent differences of vagus nerve branching may be linked to the asymmetric effects of the vagus nerve. Cervical vagus nerve branching should be taken into account when identifying main trunk of the vagus nerve for implanting electrodes to minimize potential side effects or lacking therapeutic benefits of vagus nerve stimulation.
迷走神经刺激越来越多地应用于治疗癫痫、精神疾病以及潜在的慢性心力衰竭。在将迷走神经电极植入颈迷走神经后,会以不同频率观察到诸如声音改变、呼吸困难等副作用或治疗效果不佳的情况。颈迷走神经分支可能部分导致了这些影响。然而,在迷走神经刺激的背景下,尚未对迷走神经分支进行描述。
在35具尸体供体(66个颈侧)的颈动脉鞘中宏观研究颈迷走神经的分支情况。在进行X射线成像以确定颈迷走神经分支的椎体水平后,取出样本进行组织学确认神经并计算颈迷走神经的直径和横截面积。
在所有病例中,29%观察到颈迷走神经分支(单侧26%,双侧3%),所有病例均经组织学证实。右侧分支(22%)比左侧分支(12%)更常见,左侧分支发生在第四和第五椎体水平,右侧分支发生在第二至第五椎体水平。无分支的迷走神经在直径(4.79毫米对3.78毫米)和横截面积(7.24平方毫米对5.28平方毫米)方面明显大于有分支的迷走神经。
颈迷走神经分支比先前描述的要频繁得多。迷走神经分支的侧别差异可能与迷走神经的不对称效应有关。在确定用于植入电极的迷走神经主干时,应考虑颈迷走神经分支,以尽量减少迷走神经刺激的潜在副作用或治疗效果不佳的情况。