Sembrano Jonathan N, Polly David W, Ledonio Charles Gerald T, Santos Edward Rainier G
Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, MN ; Minneapolis VA Health Care System, Minneapolis, MN.
Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, MN.
Int J Spine Surg. 2012 Dec 1;6:49-54. doi: 10.1016/j.ijsp.2011.11.002. eCollection 2012.
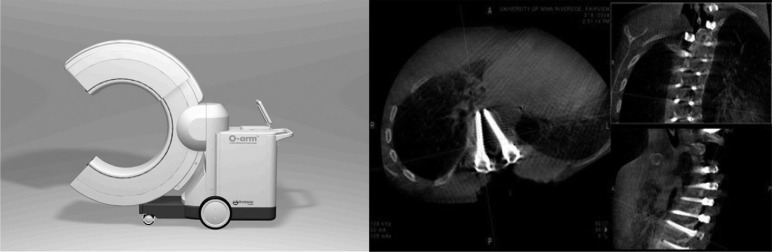
Pedicle screws are biomechanically superior over other spinal fixation devices. When improperly positioned, they lose this advantage and put adjacent structures at risk. Accurate placement is therefore critical. Postoperative computed tomography (CT) scans are the imaging gold standard and have shown malposition rates ranging from 2% to 41%. The O-arm (Medtronic Navigation, Louisville, Colorado) is an intraoperative CT scanner that may allow intervention for malpositioned screws while patients are still in the operating room. However, this has not yet been shown in clinical studies. The primary objective of this study was to assess the usefulness of the O-arm for evaluating pedicle screw position by answering the following question: What is the rate of intraoperative pedicle screw revision brought about by O-arm imaging information? A secondary question was also addressed: What is the rate of unacceptable thoracic and lumbar pedicle screw placement as assessed by intraoperative O-arm imaging?
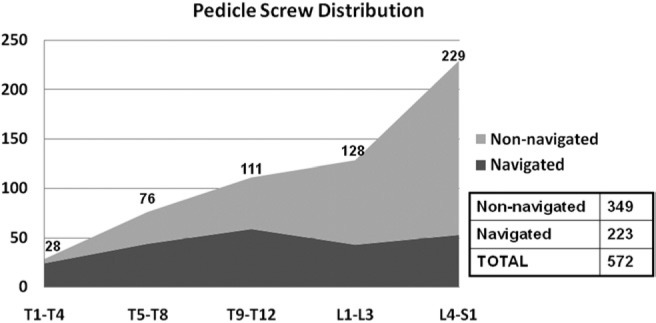
This is a case series of consecutive patients who have undergone spine surgery for which an intraoperative 3-dimensional (3D) CT scan was used to assess pedicle screw position. The study comprised 602 pedicle screws (235 thoracic and 367 lumbar/sacral) placed in 76 patients, and intraoperative 3D (O-arm) imaging was obtained to assess screw position. Action taken at the time of surgery based on imaging information was noted. An independent review of all scans was also conducted, and all screws were graded as either optimal (no breach), acceptable (breach ≤2 mm), or unacceptable (breach >2 mm). The rate of pedicle screw revision, as detected by intraoperative 3D CT scan, was determined.
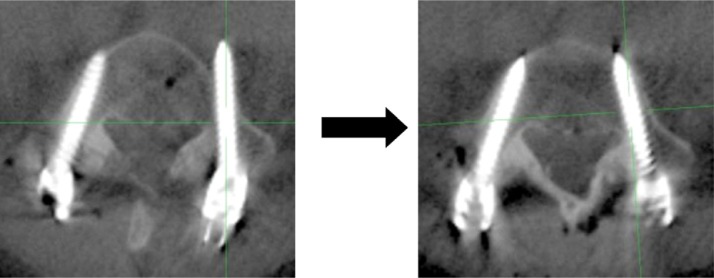
On the basis of 3D imaging information, 17 of 602 screws (2.8%) in 14 of 76 cases (18.4%) were revised at the time of surgery. On independent review of multiplanar images, 11 screws (1.8%) were found to be unacceptable, 32 (5.3%) were acceptable, and 559 (92.9%) were optimal. All unacceptable screws were revised to an optimal or acceptable position, and an additional 6 acceptable screws were revised to an optimal position. Thus, by the end of the cases, none of the 602 pedicle screws in the 76 surgical procedures was in an unacceptable position.
The new-generation intraoperative 3D imaging system (O-arm) is a useful tool that allows more accurate assessment of pedicle screw position than plain radiographs or fluoroscopy alone. It prompted intraoperative repositioning of 2.8% of pedicle screws in our series. Most importantly, it allowed identification and revision of all unacceptably placed pedicle screws without the need for reoperation.
椎弓根螺钉在生物力学方面优于其他脊柱固定装置。若位置不当,它们将失去这一优势,并使相邻结构处于危险之中。因此,准确放置至关重要。术后计算机断层扫描(CT)是成像的金标准,其显示的置钉位置不当率在2%至41%之间。O型臂(美敦力导航公司,科罗拉多州路易斯维尔)是一种术中CT扫描仪,它可能允许在患者仍在手术室时对位置不当的螺钉进行干预。然而,临床研究尚未证实这一点。本研究的主要目的是通过回答以下问题来评估O型臂在评估椎弓根螺钉位置方面的实用性:O型臂成像信息导致的术中椎弓根螺钉翻修率是多少?还提出了一个次要问题:术中O型臂成像评估的胸腰椎椎弓根螺钉放置不可接受率是多少?
这是一系列连续接受脊柱手术的患者病例,术中使用三维(3D)CT扫描评估椎弓根螺钉位置。该研究包括76例患者置入的602枚椎弓根螺钉(235枚胸椎和367枚腰椎/骶椎),并获得术中3D(O型臂)成像以评估螺钉位置。记录基于成像信息在手术时采取的行动。还对所有扫描进行了独立审查,所有螺钉被分为最佳(无突破)、可接受(突破≤2 mm)或不可接受(突破>2 mm)。确定术中3D CT扫描检测到的椎弓根螺钉翻修率。
根据3D成像信息,76例中的14例(18.4%)的602枚螺钉中有17枚(2.8%)在手术时进行了翻修。在对多平面图像进行独立审查时,发现11枚螺钉(1.8%)不可接受,32枚(5.3%)可接受,559枚(92.9%)最佳。所有不可接受的螺钉均被翻修至最佳或可接受位置,另外6枚可接受的螺钉被翻修至最佳位置。因此,在这些病例结束时,76例手术中的602枚椎弓根螺钉均未处于不可接受的位置。
新一代术中3D成像系统(O型臂)是一种有用的工具,与单纯的平片或透视相比,它能更准确地评估椎弓根螺钉位置。在我们的系列研究中,它促使2.8%的椎弓根螺钉在术中重新定位。最重要的是,它能够识别并翻修所有放置位置不可接受的椎弓根螺钉,而无需再次手术。