Kousoulas Lampros, Vondran Florian W R, Syryca Paulina, Klempnauer Juergen, Schrem Harald, Lehner Frank
General, Visceral and Transplant Surgery, Hanover Medical School, 30625 Hanover, Germany.
J Transplant. 2015;2015:712049. doi: 10.1155/2015/712049. Epub 2015 Feb 1.
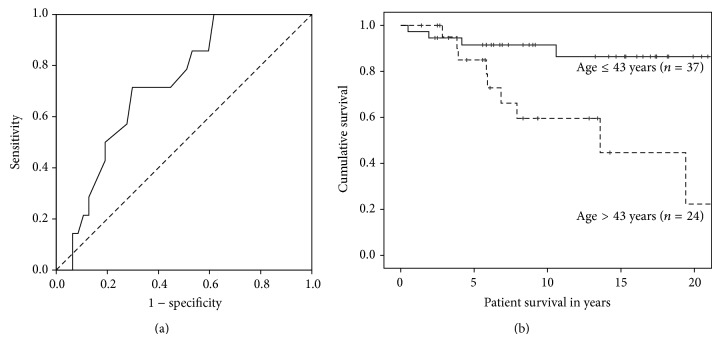
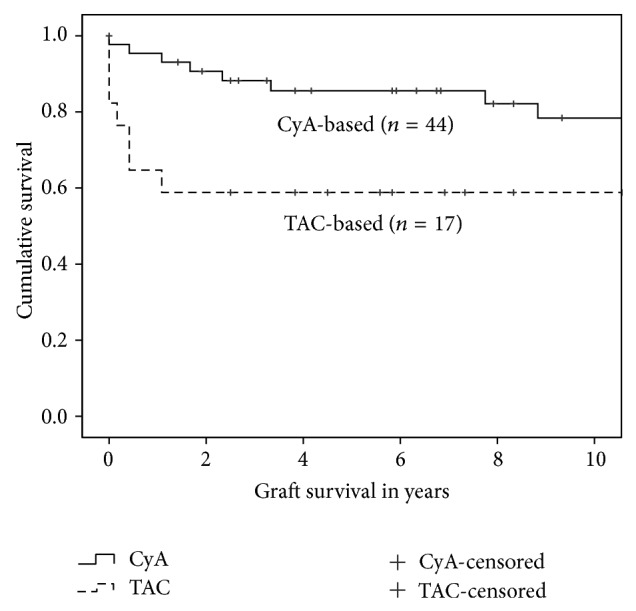
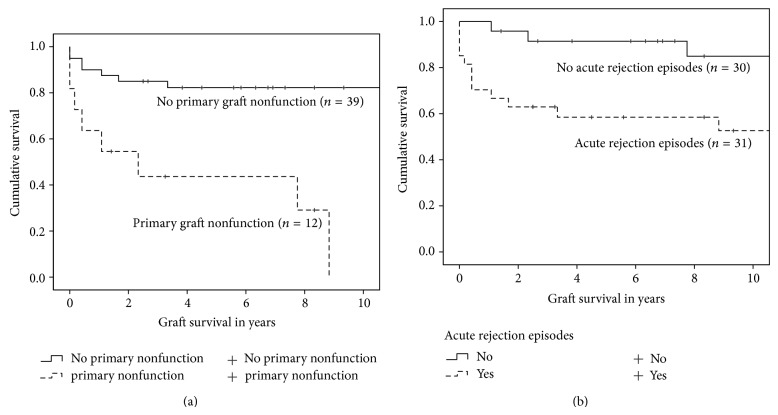
Renal transplantation is the treatment of choice for patients suffering end-stage renal disease, but as the long-term renal allograft survival is limited, most transplant recipients will face graft loss and will be considered for a retransplantation. The goal of this study was to evaluate the patient and graft survival of the 61 renal transplant recipients after second or subsequent renal transplantation, transplanted in our institution between 1990 and 2010, and to identify risk factors related to inferior outcomes. Actuarial patient survival was 98.3%, 94.8%, and 88.2% after one, three, and five years, respectively. Actuarial graft survival was 86.8%, 80%, and 78.1% after one, three, and five years, respectively. Risk-adjusted analysis revealed that only age at the time of last transplantation had a significant influence on patient survival, whereas graft survival was influenced by multiple immunological and surgical factors, such as the number of HLA mismatches, the type of immunosuppression, the number of surgical complications, need of reoperation, primary graft nonfunction, and acute rejection episodes. In conclusion, third and subsequent renal transplantation constitute a valid therapeutic option, but inferior outcomes should be expected among elderly patients, hyperimmunized recipients, and recipients with multiple operations at the site of last renal transplantation.
肾移植是终末期肾病患者的首选治疗方法,但由于肾移植长期存活受限,大多数移植受者将面临移植肾失功,并需要考虑再次移植。本研究的目的是评估1990年至2010年间在本机构接受第二次或后续肾移植的61例肾移植受者的患者和移植肾存活率,并确定与不良结局相关的危险因素。术后1年、3年和5年的患者精算生存率分别为98.3%、94.8%和88.2%。术后1年、3年和5年的移植肾精算生存率分别为86.8%、80%和78.1%。风险调整分析显示,仅末次移植时的年龄对患者生存率有显著影响,而移植肾存活率受多种免疫和手术因素影响,如HLA错配数、免疫抑制类型、手术并发症数、再次手术需求、原发性移植肾无功能和急性排斥反应发作次数。总之,第三次及后续肾移植是一种有效的治疗选择,但老年患者、高敏受者以及末次肾移植部位接受多次手术的受者可能预后较差。