Gebhard Catherine, Fuchs Tobias A, Stehli Julia, Gransar Heidi, Berman Daniel S, Budoff Matthew J, Achenbach Stephan, Al-Mallah Mouaz, Andreini Daniele, Cademartiri Filippo, Callister Tracy Q, Chang Hyuk-Jae, Chinnaiyan Kavitha M, Chow Benjamin J W, Cury Ricardo C, Delago Augustin, Gomez Millie J, Hadamitzky Martin, Hausleiter Joerg, Hindoyan Niree, Feuchtner Gudrun, Kim Yong-Jin, Leipsic Jonathon, Lin Fay Y, Maffei Erica, Pontone Gianluca, Raff Gilbert, Shaw Leslee J, Villines Todd C, Dunning Allison M, Min James K, Kaufmann Philipp A
Department of Nuclear Medicine, University Hospital Zurich and University of Zurich, Zurich, Switzerland.
Departments of Imaging and Medicine, Cedars-Sinai Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
Eur Heart J Cardiovasc Imaging. 2015 Aug;16(8):853-62. doi: 10.1093/ehjci/jeu314. Epub 2015 Mar 4.
Coronary computed tomographic angiography (CCTA) has become an important tool for non-invasive diagnosis of coronary artery disease (CAD). Coronary dominance can be assessed by CCTA; however, the predictive value of coronary dominance is controversially discussed. The aim of this study was to evaluate the prevalence and prognosis of coronary dominance in a large prospective, international multicentre cohort of patients undergoing CCTA.
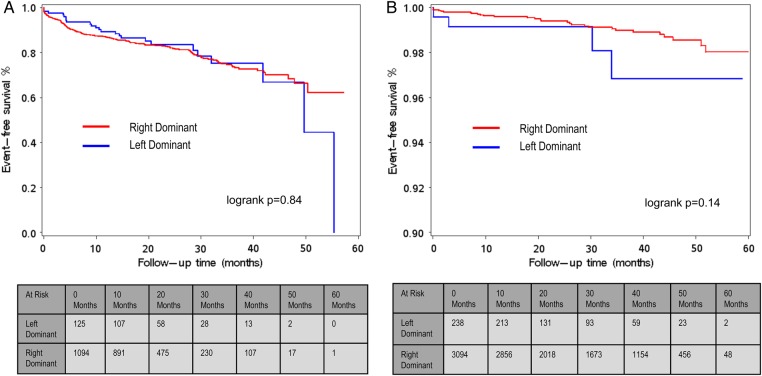
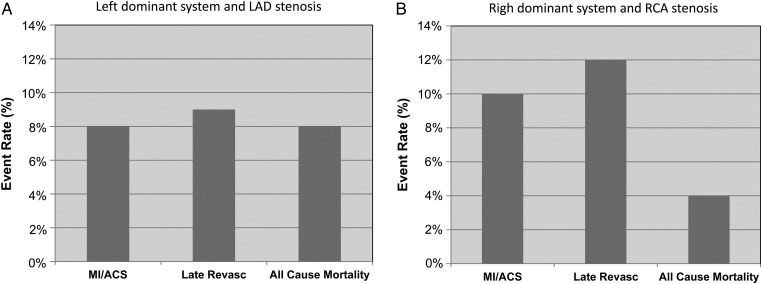
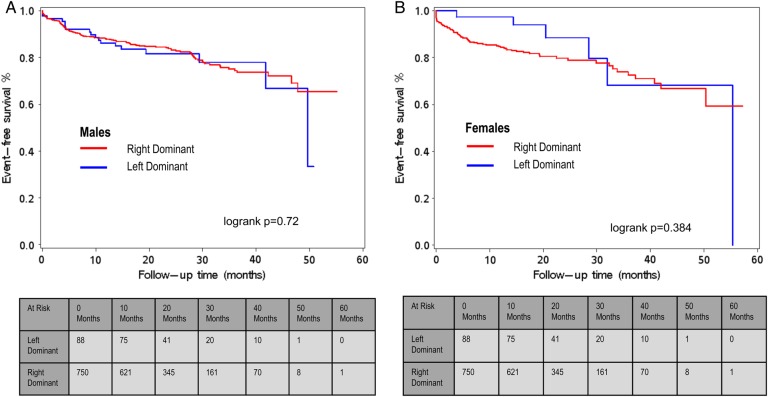
The study population consisted of 6382 patients with or without CAD (47% females, 53% males, mean age 56.9 ± 12.3 years) who underwent CCTA and were followed over a period of 60 months. Right or left coronary dominance was determined. Right dominance was present in 91% (n = 5817) and left in 9% (n = 565) of the study population. At the end of follow-up, outcome in patients with obstructive CAD (>50% luminal stenosis) and right dominance was similar compared with patients with left dominance [hazard ratio (HR) 0.46, 95% CI 0.16-1.32, P = 0.15]. Furthermore, no differences were observed for the type of coronary dominance in patients with non-obstructive CAD (HR 0.95, 95% CI 0.41-2.21, P = 0.8962) or normal coronary arteries (HR 1.04, 95% CI 0.68-1.59, P = 0.9). Subgroup analysis in patients with left main disease revealed an elevated hazard of the combined endpoint for left dominance (HR 6.45, 95% CI 1.66-25.0, P = 0.007), but not for right dominance.
In our study population, survival after 5 years of follow-up did not differ significantly between patients with left or right coronary dominance. Thus, assessment of coronary vessel dominance by CCTA may not enhance risk stratification in patients with normal coronary arteries or obstructive CAD, but may add prognostic information for specific subpopulations.
冠状动脉计算机断层血管造影(CCTA)已成为冠状动脉疾病(CAD)无创诊断的重要工具。CCTA可评估冠状动脉优势;然而,冠状动脉优势的预测价值存在争议。本研究的目的是评估接受CCTA的大型前瞻性国际多中心队列患者中冠状动脉优势的患病率和预后。
研究人群包括6382例有或无CAD的患者(47%为女性,53%为男性,平均年龄56.9±12.3岁),这些患者接受了CCTA并随访60个月。确定右冠状动脉优势或左冠状动脉优势。研究人群中91%(n = 5817)为右冠状动脉优势,9%(n = 565)为左冠状动脉优势。随访结束时,阻塞性CAD(管腔狭窄>50%)且为右冠状动脉优势的患者与左冠状动脉优势的患者的结局相似[风险比(HR)0.46,95%置信区间(CI)0.16 - 1.32,P = 0.15]。此外,非阻塞性CAD患者(HR 0.95,95% CI 0.41 - 2.21,P = 0.8962)或冠状动脉正常的患者(HR 1.04,95% CI 0.68 - 1.59,P = 0.9)在冠状动脉优势类型上未观察到差异。对左主干疾病患者的亚组分析显示,左冠状动脉优势患者联合终点的风险升高(HR 6.45,95% CI 1.66 - 25.0,P = 0.007),但右冠状动脉优势患者未升高。
在我们的研究人群中,随访5年后左冠状动脉优势和右冠状动脉优势患者的生存率无显著差异。因此,通过CCTA评估冠状动脉优势可能不会增强冠状动脉正常或阻塞性CAD患者的风险分层,但可能为特定亚组人群提供预后信息。