Gladstone Melissa, Oliver Clare, Van den Broek Nynke
Department of Women and Children's Health, Institute of Translational Medicine, University of Liverpool, Alder Hey NHS Foundation Trust, Liverpool, United Kingdom.
Centre for Maternal and Newborn Health, Liverpool School of Tropical Medicine, Liverpool, United Kingdom.
PLoS One. 2015 Mar 20;10(3):e0120566. doi: 10.1371/journal.pone.0120566. eCollection 2015.
Premature birth is the leading cause of neonatal death and second leading in children under 5. Information on outcomes of preterm babies surviving the early neonatal period is sparse although it is considered a major determinant of immediate and long-term morbidity.
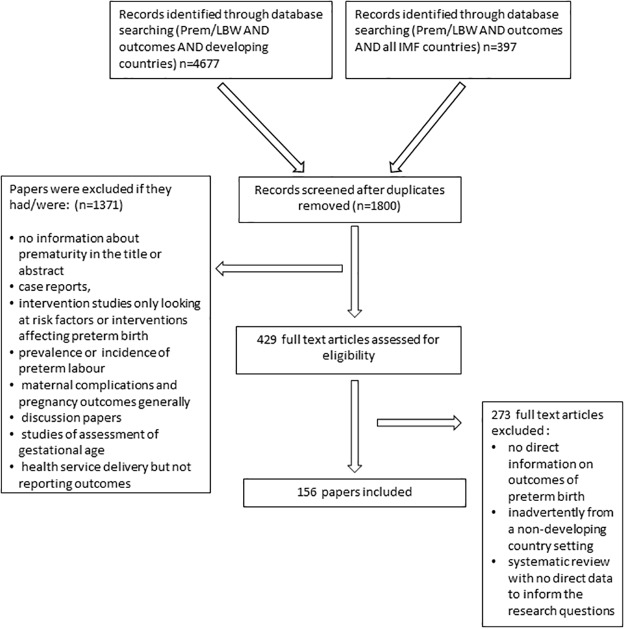
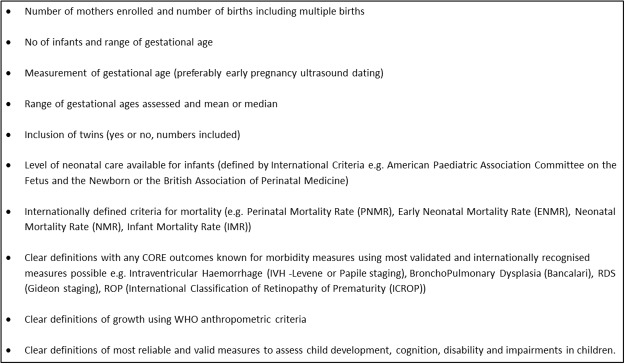
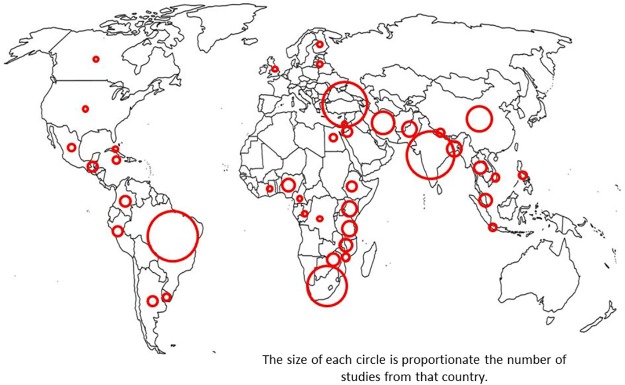
Systematic review of studies reporting outcomes for preterm babies in low and middle income settings was conducted using electronic databases, citation tracking, expert recommendations and "grey literature". Reviewers screened titles, abstracts and articles. Data was extracted using inclusion and exclusion criteria, study site and facilities, assessment methods and outcomes of mortality, morbidity, growth and development. The Child Health Epidemiology Reference Group criteria (CHERG) were used to assess quality.
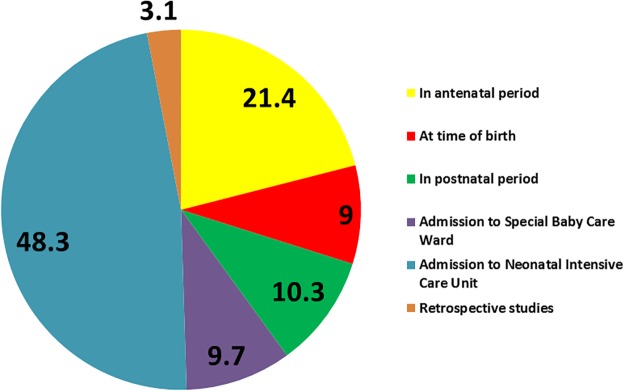
Of 197 eligible publications, few (10.7%) were high quality (CHERG). The majority (83.3%) report on the outcome of a sample of preterm babies at time of birth or admission. Only 16.0% studies report population-based data using standardised mortality definitions. In 50.5% of studies, gestational age assessment method was unclear. Only 15.8% followed-up infants for 2 years or more. Growth was reported using standardised definitions but recommended morbidity definitions were rarely used. The criteria for assessment of neurodevelopmental outcomes was variable with few standardised tools - Bayley II was used in approximately 33% of studies, few studies undertook sensory assessments.
To determine the relative contribution of preterm birth to the burden of disease in children and to inform the planning of healthcare interventions to address this burden, a renewed understanding of the assessment and documentation of outcomes for babies born preterm is needed. More studies assessing outcomes for preterm babies who survive the immediate newborn period are needed. More consistent use of data is vital with clear and aligned definitions of health outcomes in newborn (preterm or term) and intervention packages aimed to save lives and improve health.
早产是新生儿死亡的主要原因,在5岁以下儿童死亡原因中位列第二。尽管早产被认为是近期和长期发病的主要决定因素,但关于早产婴儿度过新生儿早期后的结局信息却很匮乏。
通过电子数据库、引文追踪、专家建议和“灰色文献”,对报告低收入和中等收入环境下早产婴儿结局的研究进行系统综述。评审人员对标题、摘要和文章进行筛选。使用纳入和排除标准、研究地点和设施、评估方法以及死亡率、发病率、生长发育结局等提取数据。采用儿童健康流行病学参考组标准(CHERG)评估质量。
在197篇符合条件的出版物中,高质量(CHERG)的很少(10.7%)。大多数(83.3%)报告的是早产婴儿出生时或入院时样本的结局。只有16.0%的研究使用标准化死亡率定义报告基于人群的数据。在50.5%的研究中,胎龄评估方法不明确。只有15.8%的研究对婴儿进行了2年或更长时间的随访。生长情况按照标准化定义报告,但很少使用推荐的发病率定义。神经发育结局的评估标准各不相同,标准化工具很少——约33%的研究使用贝利婴幼儿发展量表第二版,很少有研究进行感官评估。
为了确定早产对儿童疾病负担的相对影响,并为应对这一负担的医疗保健干预措施规划提供信息,需要重新认识早产婴儿结局的评估和记录。需要更多研究评估度过新生儿期的早产婴儿的结局。更一致地使用数据至关重要,要对新生儿(早产或足月)的健康结局有清晰且一致的定义,并制定旨在挽救生命和改善健康的干预方案。