Safroneeva Ekaterina, Vavricka Stephan R, Fournier Nicolas, Straumann Alex, Rogler Gerhard, Schoepfer Alain M
*Institute of Social and Preventive Medicine, University of Bern, Bern, Switzerland; †Division of Gastroenterology and Hepatology, University Hospital Zurich, Zurich, Switzerland; ‡Division of Gastroenterology and Hepatology, Stadtspital Triemli, Zurich, Switzerland; §Institute of Social and Preventive Medicine, Centre Hospitalier Universitaire Vaudois et Université de Lausanne, Lausanne, Switzerland; ‖Division of Gastroenterology and Hepatology, University Hospital Basel, Basel, Switzerland; and ¶Division of Gastroenterology and Hepatology, Centre Hospitalier Universitaire Vaudois et Université de Lausanne, Lausanne, Switzerland.
Inflamm Bowel Dis. 2015 Jun;21(6):1348-58. doi: 10.1097/MIB.0000000000000368.
Physicians traditionally treat ulcerative colitis (UC) using a step-up approach. Given the paucity of data, we aimed to assess the cumulative probability of UC-related need for step-up therapy and to identify escalation-associated risk factors.
Patients with UC enrolled into the Swiss IBD Cohort Study were analyzed. The following steps from the bottom to the top of the therapeutic pyramid were examined: (1) 5-aminosalicylic acid and/or rectal corticosteroids, (2) systemic corticosteroids, (3) immunomodulators (IM) (azathioprine, 6-mercaptopurine, methotrexate), (4) TNF antagonists, (5) calcineurin inhibitors, and (6) colectomy.
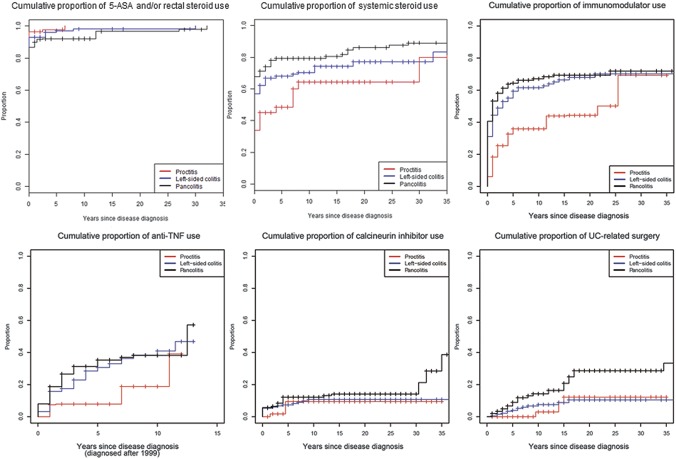
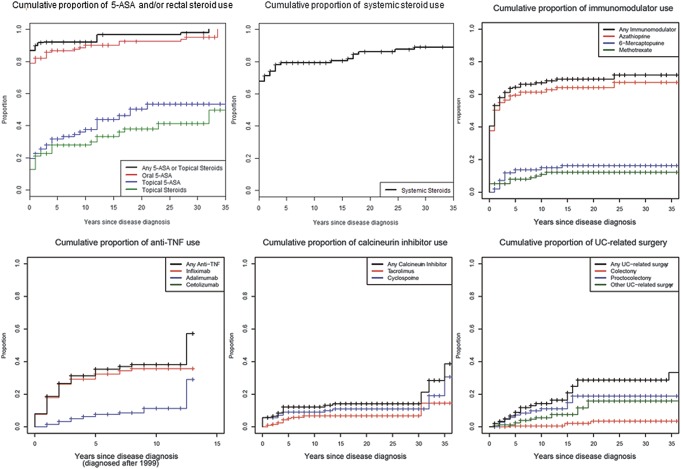
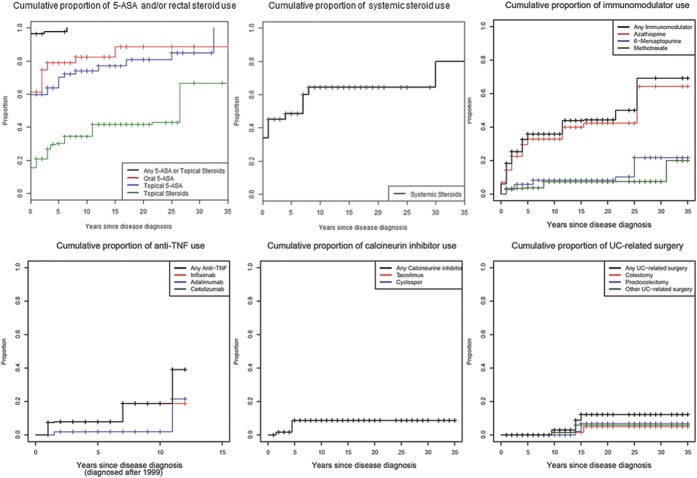
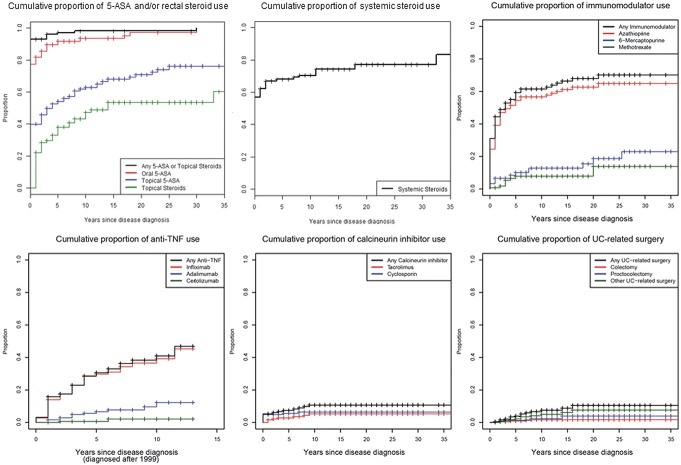
Data on 996 patients with UC with a median disease duration of 9 years were examined. The point estimates of cumulative use of different treatments at years 1, 5, 10, and 20 after UC diagnosis were 91%, 96%, 96%, and 97%, respectively, for 5-ASA and/or rectal corticosteroids, 63%, 69%, 72%, and 79%, respectively, for systemic corticosteroids, 43%, 57%, 59%, and 64%, respectively, for IM, 15%, 28%, and 35% (up to year 10 only), respectively, for TNF antagonists, 5%, 9%, 11%, and 12%, respectively, for calcineurin inhibitors, 1%, 5%, 9%, and 18%, respectively, for colectomy. The presence of extraintestinal manifestations and extended disease location (at least left-sided colitis) were identified as risk factors for step-up in therapy with systemic corticosteroids, IM, TNF antagonists, calcineurin inhibitors, and surgery. Cigarette smoking at diagnosis was protective against surgery.
The presence of extraintestinal manifestations, left-sided colitis, and extensive colitis/pancolitis at the time of diagnosis were associated with use of systemic corticosteroids, IM, TNF antagonists, calcineurin inhibitors, and colectomy during the disease course.
医生传统上采用逐步升级的方法治疗溃疡性结肠炎(UC)。鉴于数据有限,我们旨在评估UC相关的逐步升级治疗需求的累积概率,并确定与升级相关的风险因素。
对纳入瑞士炎症性肠病队列研究的UC患者进行分析。研究了治疗金字塔从底部到顶部的以下步骤:(1)5-氨基水杨酸和/或直肠皮质类固醇,(2)全身皮质类固醇,(3)免疫调节剂(IM)(硫唑嘌呤、6-巯基嘌呤、甲氨蝶呤),(4)肿瘤坏死因子拮抗剂,(5)钙调神经磷酸酶抑制剂,以及(6)结肠切除术。
检查了996例UC患者的数据,疾病中位病程为9年。UC诊断后第1年、第5年、第10年和第20年不同治疗的累积使用点估计分别为:5-氨基水杨酸和/或直肠皮质类固醇为91%、96%、96%和97%,全身皮质类固醇分别为63%、69%、72%和79%,IM分别为43%、57%、59%和64%,肿瘤坏死因子拮抗剂分别为15%、28%和35%(仅到第10年),钙调神经磷酸酶抑制剂分别为5%、9%、11%和12%,结肠切除术分别为1%、5%、9%和18%。肠外表现的存在和病变范围扩大(至少左侧结肠炎)被确定为全身皮质类固醇、IM、肿瘤坏死因子拮抗剂、钙调神经磷酸酶抑制剂和手术治疗升级的风险因素。诊断时吸烟对手术有保护作用。
诊断时存在肠外表现、左侧结肠炎以及广泛性结肠炎/全结肠炎与疾病过程中使用全身皮质类固醇、IM、肿瘤坏死因子拮抗剂、钙调神经磷酸酶抑制剂和结肠切除术有关。