Kohler Betsy A, Sherman Recinda L, Howlader Nadia, Jemal Ahmedin, Ryerson A Blythe, Henry Kevin A, Boscoe Francis P, Cronin Kathleen A, Lake Andrew, Noone Anne-Michelle, Henley S Jane, Eheman Christie R, Anderson Robert N, Penberthy Lynne
North American Association of Central Cancer Registries, Springfield, IL (BAK, RLS, KAH, FPB); National Cancer Institute, Bethesda, MD (NH, KAC, AMN, LP); American Cancer Society, Atlanta, GA (AJ); Centers for Disease Control and Prevention, Atlanta, GA (ABR, SJH, CRE); Temple University Department of Geography, Philadelphia, PA (KAH); New York State Cancer Registry, NY (FPB); Information Management Services, Inc., Rockville, MD (AL); National Center for Health Statistics, Hyattsville, MD (RNA).
J Natl Cancer Inst. 2015 Mar 30;107(6):djv048. doi: 10.1093/jnci/djv048. Print 2015 Jun.
The American Cancer Society (ACS), Centers for Disease Control and Prevention (CDC), National Cancer Institute (NCI), and North American Association of Central Cancer Registries (NAACCR) collaborate annually to produce updated, national cancer statistics. This Annual Report includes a focus on breast cancer incidence by subtype using new, national-level data.
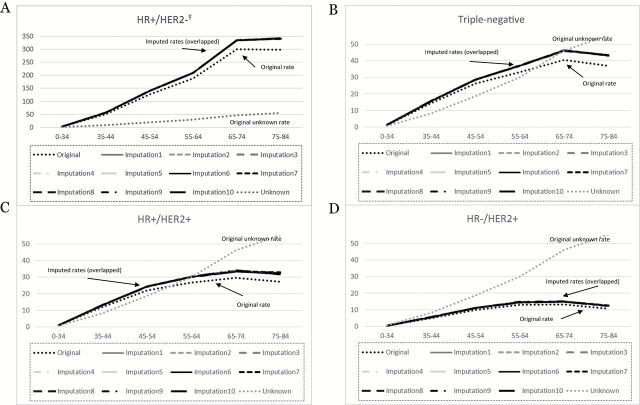
Population-based cancer trends and breast cancer incidence by molecular subtype were calculated. Breast cancer subtypes were classified using tumor biomarkers for hormone receptor (HR) and human growth factor-neu receptor (HER2) expression.
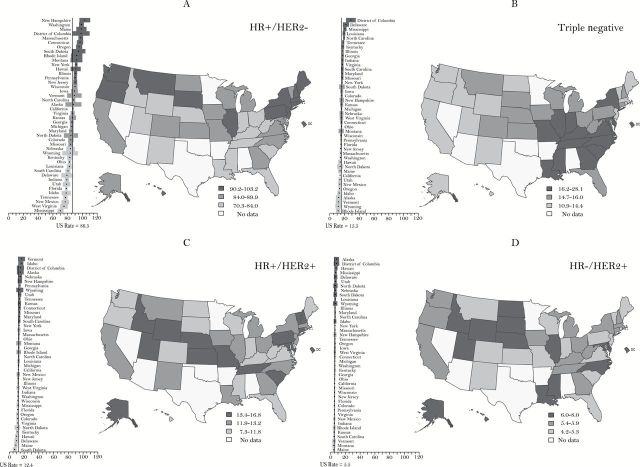
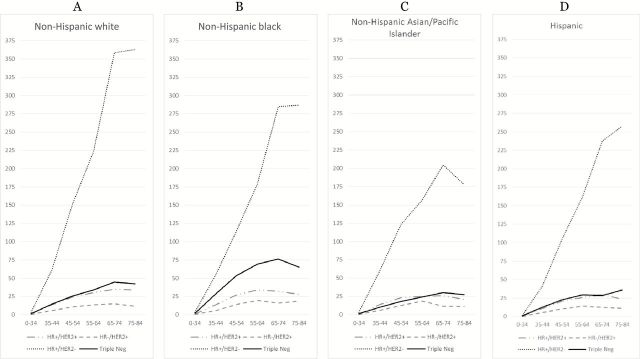
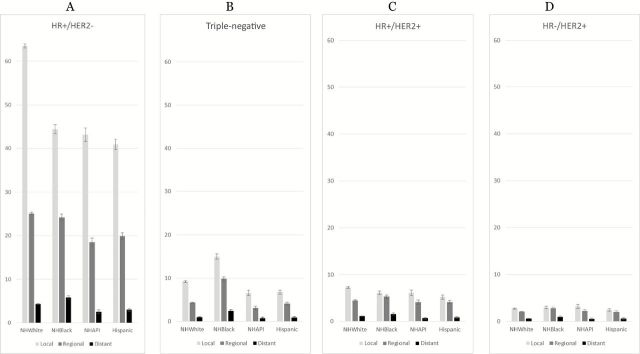
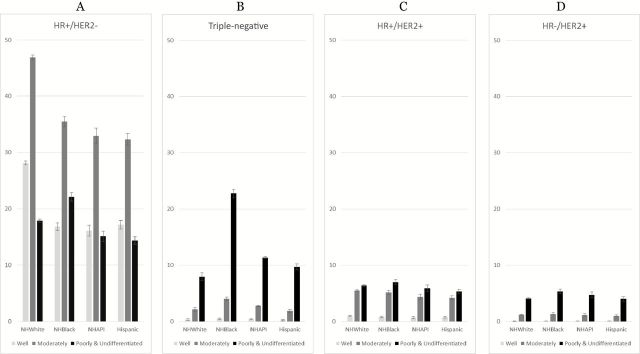
Overall cancer incidence decreased for men by 1.8% annually from 2007 to 2011 [corrected]. Rates for women were stable from 1998 to 2011. Within these trends there was racial/ethnic variation, and some sites have increasing rates. Among children, incidence rates continued to increase by 0.8% per year over the past decade while, like adults, mortality declined. HR+/HER2- breast cancers, the subtype with the best prognosis, were the most common for all races/ethnicities with highest rates among non-Hispanic white women, local stage cases, and low poverty areas (92.7, 63.51, and 98.69 per 100000 non-Hispanic white women, respectively). HR+/HER2- breast cancer incidence rates were strongly, positively correlated with mammography use, particularly for non-Hispanic white women (Pearson 0.57, two-sided P < .001). Triple-negative breast cancers, the subtype with the worst prognosis, were highest among non-Hispanic black women (27.2 per 100000 non-Hispanic black women), which is reflected in high rates in southeastern states.
Progress continues in reducing the burden of cancer in the United States. There are unique racial/ethnic-specific incidence patterns for breast cancer subtypes; likely because of both biologic and social risk factors, including variation in mammography use. Breast cancer subtype analysis confirms the capacity of cancer registries to adjust national collection standards to produce clinically relevant data based on evolving medical knowledge.
美国癌症协会(ACS)、疾病控制与预防中心(CDC)、国家癌症研究所(NCI)以及北美中央癌症登记协会(NAACCR)每年都会合作编制最新的全国癌症统计数据。本年度报告重点关注使用新的国家级数据按亚型划分的乳腺癌发病率。
计算基于人群的癌症趋势以及按分子亚型划分的乳腺癌发病率。乳腺癌亚型通过激素受体(HR)和人类生长因子神经受体(HER2)表达的肿瘤生物标志物进行分类。
从2007年到2011年[校正后],男性总体癌症发病率每年下降1.8%。1998年到2011年女性发病率保持稳定。在这些趋势中存在种族/族裔差异,并且一些部位的发病率有所上升。在儿童中,过去十年发病率继续以每年0.8%的速度上升,而与成年人一样,死亡率有所下降。HR+/HER2-乳腺癌是预后最好的亚型,在所有种族/族裔中最为常见,在非西班牙裔白人女性、局部阶段病例以及低贫困地区发病率最高(每10万名非西班牙裔白人女性中分别为92.7、63.51和98.69例)。HR+/HER2-乳腺癌发病率与乳房X线摄影检查的使用呈强正相关,尤其是对于非西班牙裔白人女性(Pearson相关系数为0.57,双侧P <.001)。三阴性乳腺癌是预后最差的亚型,在非西班牙裔黑人女性中发病率最高(每10万名非西班牙裔黑人女性中为27.2例),这在东南部各州的高发病率中有所体现。
美国在减轻癌症负担方面继续取得进展。乳腺癌亚型存在独特的种族/族裔特异性发病模式;这可能是由于生物学和社会风险因素共同作用的结果,包括乳房X线摄影检查使用情况的差异。乳腺癌亚型分析证实了癌症登记机构根据不断发展的医学知识调整国家收集标准以生成临床相关数据的能力。